I’m afraid I don’t have any clinical information to accompany this ECG, but all I’d like is a description of the rhythm, with as much information and explanation as you can provide.
ANSWER
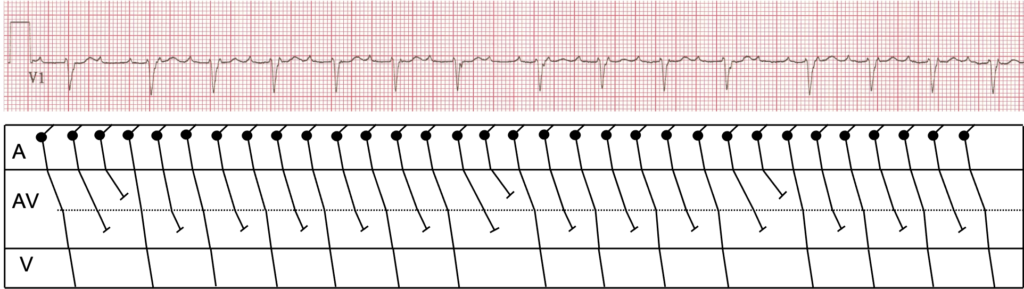
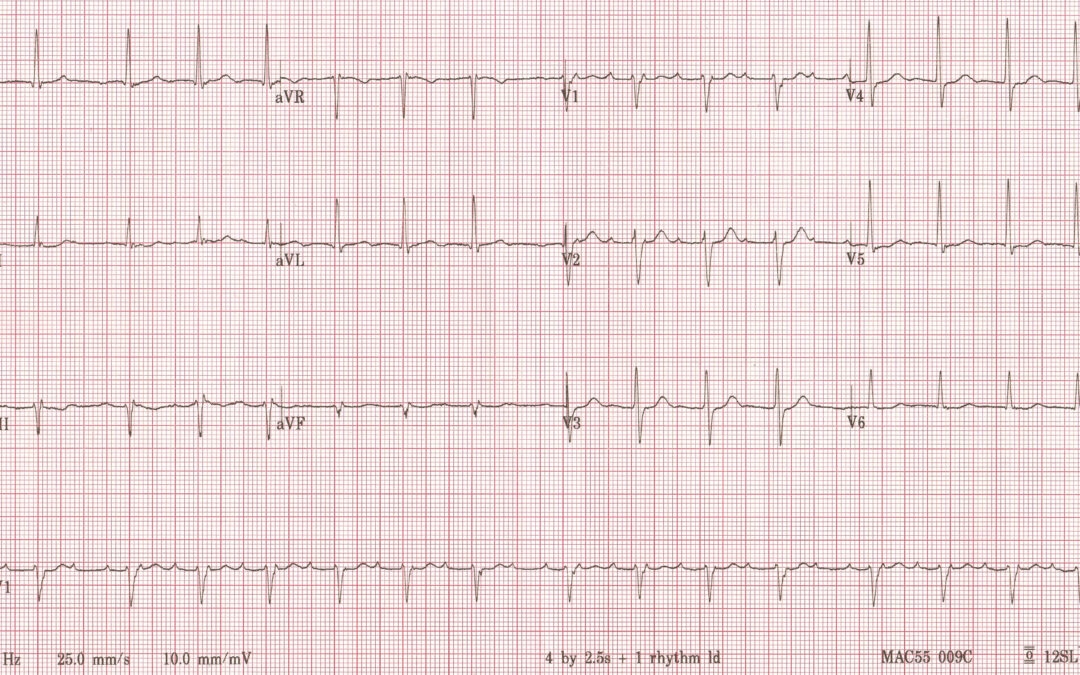
OK, first things first. The P waves are of low amplitude in most leads and negative in I and aVL, although strongly positive in V1 and V2, and the atrial rate is 200 bpm. This is because there is an atrial tachycardia. The ventricular rate is irregular and far less than 200 bpm, so there is AV block. It might be tempting just to describe this as atrial tachycardia with variable block but I think we can go a bit further. The PR interval of the conducted beats increases gradually until there is a pause, after which the PR interval is shorter, but this cannot be described as simple Wenckebach block because there are never two consecutive P waves that conduct: every conducted P wave is followed by one or two non-conducted P waves, and this is most likely because of dual-level AV nodal block. Dual-level AV nodal block is commonly seen in atrial tachycardia and atrial flutter and accounts for many of the ECGs that we might describe as showing ‘atrial flutter with variable block’. The accompanying laddergram shows how the dual-level AV nodal block might be operating in this case. It shows long Wenckebach sequences in the upper AV node, with those impulses that make it to the lower AV node showing 2:1 block out of the lower AV node and into the ventricles.
Thanks to everyone who contributed to the discussion. Everyone got at least part of the way to the solution and Scott Walton additionally recognised the dual-level AV nodal block.
Happy Christmas!
Hi Dave
I’ll give this a go! At first I thought this was maybe Wenckebach but then on further inspection I could see a regular P rate with some in the QRS’s. Also in Lead I the P waves appear negative so I thought then this might be an atrial tachy. So, I think this is an atrial tachy at a rate of 190bpm. The R-R interval is irregular so I think there is a variable conduction. I can’t assess the 1st QRS as can’t see the baseline before but I think the 2nd QRS is 3:1 conduction, 3rd-7th QRS is 2:1 conduction. The 8th QRS is 3:1 conduction and 9th-11th are 2:1 conduction. The 12th QRS is 3:1 conduction and 13-14th are 2:1 conduction.
Thanks Beth. I think you’re on the right lines, and you’ve certainly appreciated the complexities of the rhythm, but is there a simple(ish) unified explanation that will account for everything we see?
Mobitz 1 / Wenkebach
Thanks Victoria. Mobitz I is certainly a partial explanation, but is this typical Mobitz I, and what is the atrial rhythm?
Sustained atrial tachycardia, likely re-entrant, with 2:1 conduction and concurrent PR lengthening, with a typical Wenckebach pattern, which becomes atypical as there are therefore two consecutive non-conducted P-waves within each prolonged RR interval.
Dual-level AV nodal block, or possibly combined nodal and Hisian blocks – the latter being less likely given the normal intraventricular conduction pattern.
Good ECG: I look forward to the laddergram.
Astute comments, as always, Scott. A laddergram will appear in due course!
There is a supraventricular tachycardia (atrial rate 190bpm), as I think I can see pseudo R and S waves, I would say this is AVNRT. However, this is a very slow ventricular rate for AVNRT; it looks like every other P wave is conducted. There is also progressive PR lengthening, followed by a dropped beat (ie: the beat expected to conduct in the 2:1 conduction block pattern doesn’t conduct), therefore there is Wenckebach. The dropped beat caused by Wenckebach ‘resets’ the 2:1 conduction block pattern, hence there are 2 consecutive non-conducted atrial beats before each dropped beat. I’m not sure if you can have Wenckebach and 2:1 conduction block, but that’s the pattern I see!
Thanks for your comments, Naomi. is it possible to have an AVNRT with Wenckebach block and 2:1 block? Exactly what mechanism would you put forward to explain this? Maybe there’s a slightly simpler (but not very simple) explanation!
I’m not sure I know enough about ECGs to give a complete answer! There is an atrial tachycardia (atrial rate 190bpm), with 2:1 conduction as well as Wenckebach.
The dropped beat caused by Wenckebach ‘resets’ the 2:1 conduction pattern, hence there are 2 consecutive non-conducted atrial beats before each dropped beat.
I would guess that the dropped beat caused by the Wenckebach allows time for the AVN to come out of refractory, meaning that the next atrial beat can be conducted?
Thanks, Naomi. I think you’re very much on the right lines but not quite there. I do agree with much of what you say and will offer my explanation within the next couple of days.