Let’s start this new feature with the challenge of a slightly tricky arrhythmia. See if you can describe fully what’s happening here. Warning: it’s very unlikely that a simple 3 or 4 word description will suffice! Tell us what you think it is in the comments section below.
Dr Dave Richley, Associate Lecturer, Newcastle University
Congratulations to James Bongart – Trainee Cardiac Physiologist at Nottingham University Hospitals NHS Trust. The previous month’s ECG was Sinus Rhythm with 1st degree AV block, the PR interval being very long indeed (480ms).
James Bongart – Answer to ECG July 2020
Answer: Intermittent BBB and varying degree of AVB (mainly 2:1 and CHB).
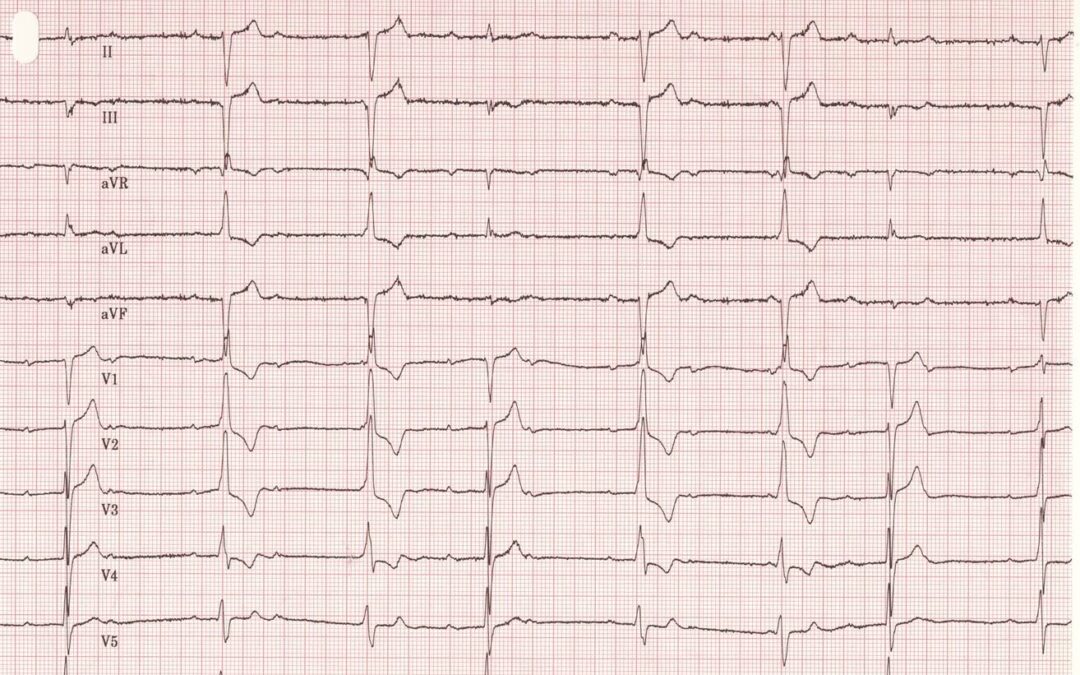
First QRS complex has a normal morphology with a PR interval of around 400ms (1st degree AVB). A second P wave follows the T wave, which is then followed by another P wave (2:1 AVB) and a QRS complex with what looks like an rSr morphology, indicative of RBBB, with a PR interval of around 280ms. A P wave falls after this T wave, but the next P wave looks like it falls in the upstroke of the R wave. This could be indicative of CHB. This is then followed by a normal QRS with 1st degree AVB.
The fifth complex is again the BBB morphology with 1st degree AVB, with a P wave falling after the T wave, and the 6th complex having a short PR interval with BBB morphology. The 7th complex shows normal QRS morphology with 1st degree AVB, and then there is a P wave within the T wave.
F/U: 24hr tape. Symptoms? Device therapy?
High grade AV block with ventricular escape rhythm. High grade block as opposed to CHB as QRS 1,4 and 7 have conducted normally with long PR interval. After these QRS, there is a p-wave but bundle branches are still in refractory period so don’t conduct. When no normal conduction through AV Node, ventricular escape beats fill in the gaps.
Variable AV block with variable intraventricular conduction.
Mandatory for pacing unless secondary to reversible cause.
Thanks, James, for kicking off the discussion of this arrhythmia. I think you’ve partly solved the problem, but we haven’t got the complete answer yet. You correctly point out that beat 1 is a conducted beat, then the P wave following it is blocked and you describe this as 2:1 block. You then raise the possibility of a brief episode of CHB, but complete heart block is a situation where no atrial impulses can conduct to the ventricles, no matter when in the cardiac cycle they occur, so the description isn’t really appropriate for something that lasts for a second or two.
And Scott, thanks for chipping in, but what exactly do you mean by variable block, and why does the block vary? Is there definitely varying intraventricular conduction?
To everyone following this, the apparent variation in PR interval has been described, but why should this happen? Also, some beats are described as showing a RBBB morphology, but what is the explanation for this? How exactly should we describe the AV block that we see here? It’s been described as a mixture of first degree, 2:1 and complete block, but why does it seem to vary?
A start has been made in unravelling this arrhythmia but there is more work to do! I’m looking forward to seeing more suggestions, so please post your thoughts.
Can you get a change in PR interval and RBBB from hyperkalaemia? V2 and V3 T waves on Normal QRS could be peaky?
I agree with Tony Shannon. The P waves before QRS beats 1, 4 and 7 are conducted (capture beats); the PR intervals on these beats are identical at around 400ms, and the QRS morphology appears normal.
QRS beats 2, 3, 5, 6, and 8, I think are escape beats – whether this is junctional escape with a RBBB or ventricular escape I’m never quite sure, and probably doesn’t matter. Although QRS 8 looks like a fusion between capture and escape beat.
A few years ago I wouldn’t know what to call this rhythm. I’ve heard it being described as an “almost complete heart block”. As Dave Richley points out it’s not “complete” if some of the atrial impulses are conducted. So, I believe the correct term is sinus rhythm with “high grade AV block”.
My personal approach to these rhythms is mainly a process of elimination. To rule out what it isn’t. E.g. it’s not first degree, it doesn’t fit into the second-degree type 1 type 2 categories, and it’s not strictly a complete heart block (main clue being that the rhythm is not regular). It’s then a case of trying to work out which P waves are capturing, and which ones aren’t – to do this I usually start by trying to find where the PR intervals are consistent. In this example, the change in QRS morphology also massively helps although I’ve seen high grade AV blocks where the QRS morphology doesn’t change because the escape beats have identical morphology to the capture beats (these ones can be really tricky).
I think in practice a lot of these ECGs are put in the complete heart block category and it requires pacing. That’s assuming I’m correct! Looking forward to hearing the answer…
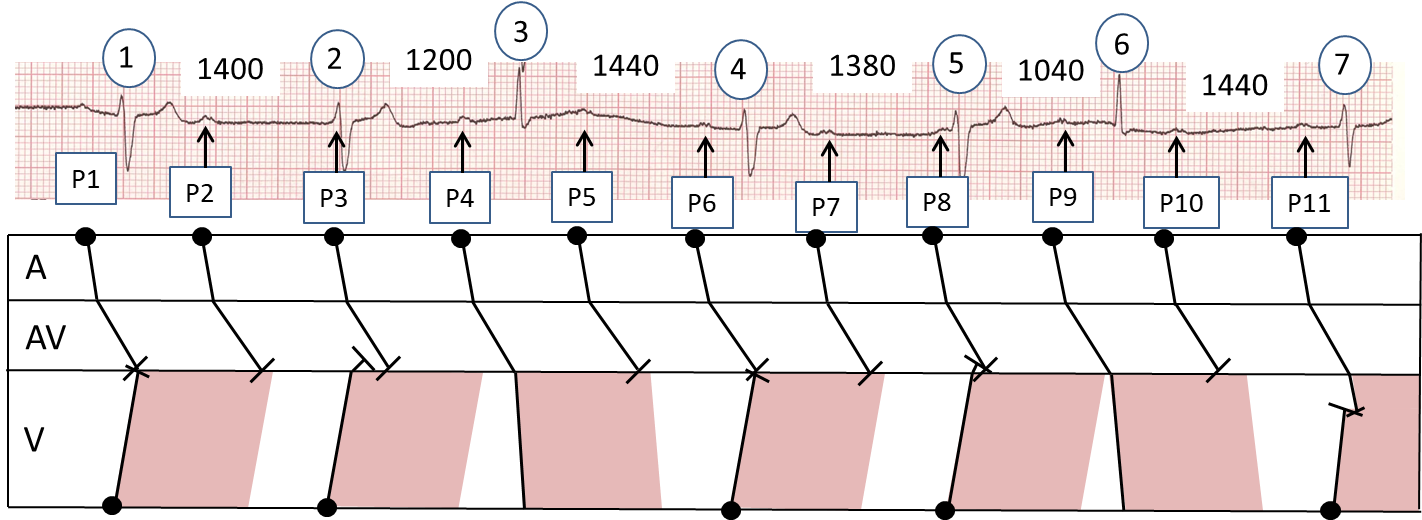
Thanks to Maxine and Tony for their insightful contributions. I think we’ve just about got this one sorted now. I’ll now detail exactly what I think is happening, but bear in mind that I could be wrong, so further contributions to the discussion are welcome. On a section of V6 from the posted ECG (only the first beat is missing from the original tracing) I have indicated all the P waves with arrows and numbered them. I’ve also numbered the QRS complexes and measured all the RR intervals in milliseconds. All references to beat numbers will refer to this picture, not the original ECG. I’ve also drawn a laddergram, which I think much better explains what’s going on than I can manage with words. If you’re interested in complex rhythms but don’t know how laddergrams work, I recommend that you learn how to use and interpret them – they’re a great aid to understanding and explanation. On the laddergram I have also indicated in pink what I think the refractory period of the ventricular muscle may be, such that if an impulse arrives at the ventricles during this period it will not conduct any further.
There is obviously some degree of AV dissociation here, as there are far more P waves than QRS complexes and the PR intervals vary. However, this is not complete heart block because the ventricular rate is irregular and there are 2 distinct QRS morphologies. Let’s go through this one beat at a time.
P1: The first sinus impulse conducts through the atria and AV node but when it arrives at the ventricles it can’t proceed any further because a ventricular focus has discharged and conducted back up towards the AV node, rendering the ventricles refractory to another activation. QRS (1) is broad and probably represents a ventricular escape beat.
P2: This sinus impulse suffers the same fate as P1 and cannot conduct past the AV node.
P3: This P wave is only just visible superimposed on the start of QRS (2). At about the same time that it appears, the ventricular escape focus discharges again after an interval of 1400 ms and QRS (2) is another ventricular escape beat. Sinus impulse P2 therefore arrives at the ventricles while they are still refractory and comes to a halt.
P4: This sinus impulse conducts down to the AV node as usual and arrives at the ventricles after the refractory period, in other words when the ventricular tissue has recovered its ability to be depolarised again. QRS (3) therefore represents a conducted or ‘capture’ beat.
P5: Again, the sinus impulse reaches the ventricles when they are refractory and is blocked.
P6: This sinus impulse also fails to conduct to the ventricles because at the same time that the sinus node discharges, so also does the ventricular focus after the escape interval of just over 1400 ms times out. The sinus impulse arrives at the ventricles to find that they have just been depolarised, to produce QRS (4) and are therefore refractory.
P7: This sinus impulse arrives at the ventricles while they are still refractory and is therefore blocked.
P8: Before this impulse reaches the ventricles, the ventricular focus discharges after its escape interval of almost 1400 ms to produce QRS (5), thus rendering the ventricles refractory to further stimulation.
P9: This sinus impulse arrives at the ventricles just after the refractory period has ended and there is therefore another capture beat (QRS (6)).
P10: Once again, the sinus impulse encounters refractory ventricular tissue and is blocked.
P11. At much the same time as the sinus node discharges, so does the ventricular focus, because its escape interval has timed out again, to produce QRS (7), but when the sinus impulse reaches the ventricles, the coast is clear – the ventricular tissue just below the His bundle is not refractory and the sinus impulse starts to conduct through the ventricles. However, before it has made much progress, this wave of depolarisation heading downwards meets the ventricular escape wavefront heading upwards with the result that the ventricles are depolarised partly as a result of the sinus impulse and partly because of the ventricular discharge. The ensuing QRS (7) is therefore a fusion beat. Although at first glance it may look similar to the ventricular escape beats, it is slightly narrower with a less deep S wave. Well done, Maxine, for spotting this!
This ECG defies classification into one of the standard categories of 1st, 2nd or 3rd degree AV block – it’s more complex than that. It could be termed high-grade AV block, which is normally defined as the occurrence of more blocked than conducted P waves, or an instance of 2 or more consecutively blocked P waves. Certainly, most of the sinus impulses here do not conduct to the ventricles, but is it accurate to say that they are all blocked? P2, P5, P7 and P10 are blocked because they occur at a time when they should be able to conduct but don’t. However, P3, P6 and P8 occur at a time when they cannot conduct simply because ventricular escape beats prevent them from doing so. These could be described as non-conducted rather than blocked P waves, because it is not disease of the conduction system that prevents their transmission, it is the presence of ventricular escape beats. This is well shown by P11 which successfully enters the ventricles, showing that it is not blocked, but it quickly encounters a simultaneous ventricular escape beat and can then proceed no further. So, some of these sinus impulses are blocked, showing that there is conduction system disease, but others are non-conducted and one is partly conducted. When trying to describe a complex arrhythmia, maybe it is more useful to first understand and then explain what seems to be going on rather than just trying to attach a standard label to it.
When faced with an ECG like this, how should you approach its analysis? There are probably a number of ways, but my attention always focuses quickly on the relatively early beats – beats (3) and (6) here – because these are often capture beats. As these beats have a different QRS morphology from the majority of the beats and because they occur after a constant PR interval of 360 ms, this confirms that they are indeed capture beats and the others, because of their constant RR interval of approximately 1400 ms and absence of any relation to P waves, are escape beats. Another early step to take is to reliably identify all the P waves, bearing in mind that some are likely to be partly or completely concealed by QRS complexes and T waves. Rigorous, methodical analysis will usually yield a plausible explanation.
Thanks you for your contribution in solving this ECG. I quite agree with James response to the ECG solution . My query is, how will this be answered in an examination. Do we have to write up as you have written?
I think it’s unlikely that you’d get an ECG like this in an exam. Did you have any particular exam in mind?