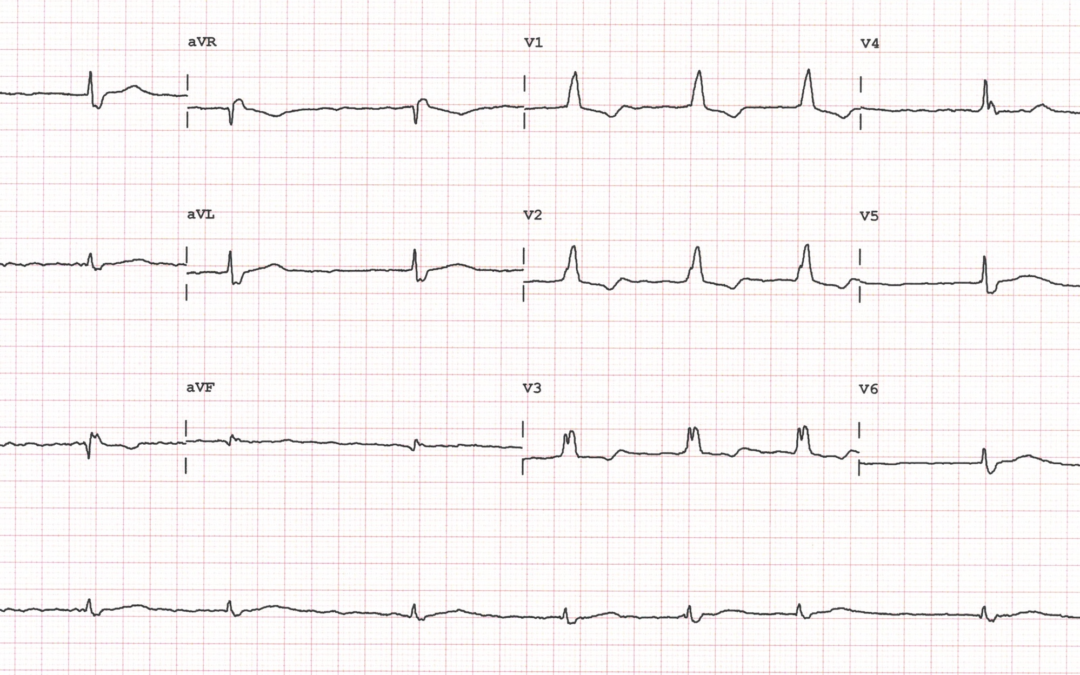
ECG 1 (Above) was recorded from an aysmptomatic 79-year old female with hypertension, for which she was taking an ACE inhibitor and a diuretic. ECG 2 (below – apologies for the size, please zoom if you can) was recorded two months later as part of a routine assessment for cancer surgery. Is there any significant difference between the two ECGs? If so, what might be the explanation?
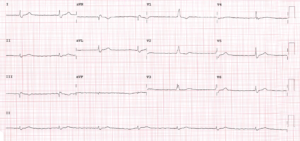
First ECG shows AF with RBBB and tendency to slow ventricular response. This in the absence of rate limiting agents with AV node effect suggest some degree of AV node disease. The second ECG shows similar QRS morphology but now with regular R-R intervals which would mean further degeneration of AV node function into high degree AV block with junctional escape (the QRS is wide but has same baseline morphology).
I agree with Francisco.
The second ECG looks like atrial fibrillation with complete heart block. Regular ventricular rhythm at approx. 42bpm. There is RBBB (same as first ECG), so I think this is a junctional escape rhythm with RBBB.
The first ECG: RBBB. I would have probably just had this down as AF with a slow to normal ventricular response approx. 42-75 bpm if I hadn’t seen second ECG. But I’m thinking maybe there are junctional escape beats in there. QRS 2, 4, 8 and 9 occur after the longest R-R intervals and have identical cycle lengths. So, I think this maybe AF with intermittent junctional escape beats. The rate at which the escape beats kick in is 42bpm, the same rate as the escape rhythm in the second ECG.
If the patient is not taking digoxin/anything that slows conduction through the AV node, I would assume that the cause is conduction disease (RBBB would also point towards that too).
Great comments from Francisco and Max. It looks as though ECG 1 shows AF with high grade AV block and, for the reasons given by Max, a mixture of conducted and junctional escape beats. Also, there is RBBB + small Q waves of unclear significance in III and aVF. ECG 2 shows AF again but now with a completely regular ventricular rate, presumably because of complete AV block and a junctional escape rhythm. Therefore, it seems that the patient has significant conduction system disease and because of this she had a permanent pacemaker implanted before proceeding to surgery.
I think this is just RBBB AND AF