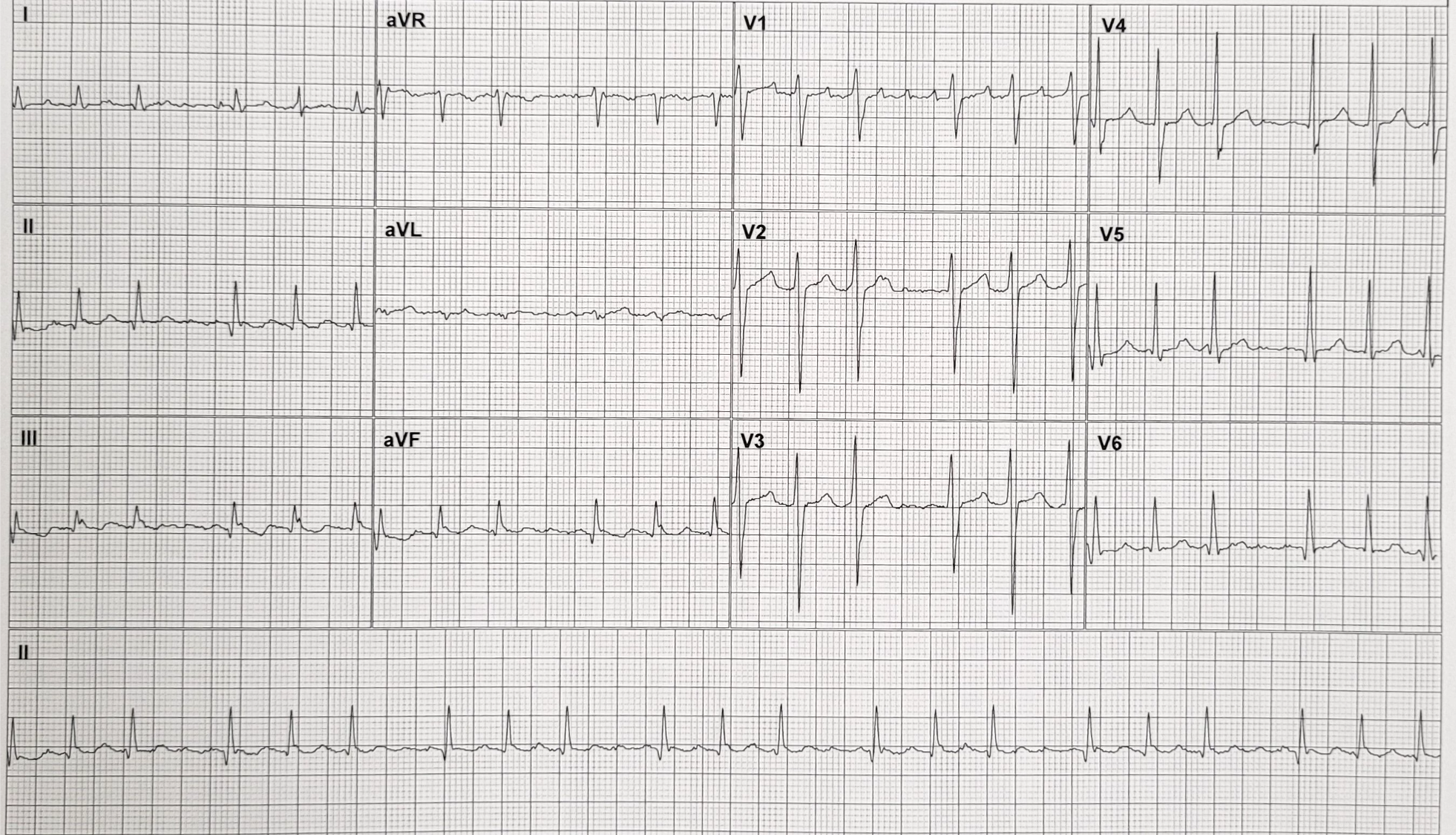
Once again, I’d like to thank Arron Pearce for my ECG of the month. This one was recorded from a 74-year-old male who presented with dyspnoea having recently undergone an ablation for atrial fibrillation.
What is the rhythm, and why do the QRS complexes occur in repeated groups of three?
Dr Dave Richley
ANSWER
NOTE: Answer added 24.04.24
First, let’s work out the atrial rhythm. It is evident, particularly from V1, that the atrial rate is very close to 300 bpm. Furthermore, if we look at the limb leads we can see that there is no section of isoelectric baseline between atrial deflections, so this is almost certainly atrial flutter, albeit perhaps a not completely typical form because of the absence of a clear ‘sawtooth’ waveform.
Next, we ’ll us turn to the conduction pattern. The QRS complexes occur in groups of three, and grouped complexes should always prompt a suspicion of Wenckebach block. But this can’t be simple Wenckebach block because if it were, with an atrial rate of 300 bpm, the ventricular would be much higher than it is here.
As Kathryn Taylor reasoned, there is probably dual-level AV nodal block. I have constructed a laddergram to illustrate exactly what I think is happening.
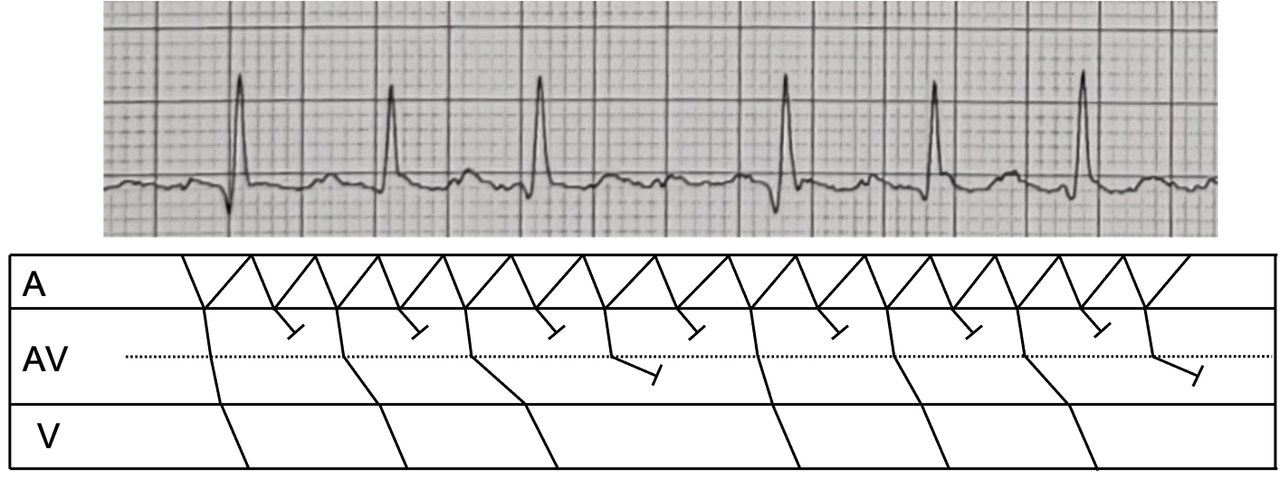
There is 2:1 block in the upper AV node with the consequence that only every other atrial impulse conducts to the lower AV node. This means that atrial impulses exit the upper AV node at a rate of about 150 bpm. There is then 4:3 Wenckebach block of these impulses in the lower AV node, meaning that only 3 of every 4 atrial impulses that make it to the lower AV node manage to conduct to the ventricles. This explains the grouping of the QRS complexes.
There also minor variations in the pattern of intraventricular conduction, the most notable example of which is the relatively deep S wave in V2 – V4 of the second QRS in every group of three. This could be regarded as a form of the Ashman phenomenon, which we have discussed previously, or simply a manifestation of slight, rate – related variation in the refractoriness of different elements of the bundle branch system.
Multi-level AV nodal block occurs frequently in atrial flutter, and occasionally in atrial tachycardia, and it explains repetitive patterns of QRS groupings, that are often described simply as atrial flutter with variable block.
Dave Richley
atrial tachycardia with variable AV conduction – Mobitz type 1 AV block (conduction 4:3)
Thanks, John. You may well be on the right lines, but is this the full explanation? What do you think is the atrial rate?
Allways great to read and see Dr Richleys, I allways learn something from you comments and EKGs. Like some have said before an atrial tachyarrhytmia, I think it is probably some form macroreentry given the distinct P-wave in V1. Looking at atrial rate around 280 bpm consistent with atrial flutter
Thank you very much, Enis. I agree with you about atrial flutter and my full explanation will appear soon.
Atrial tachycardia and wenchebach
Thanks, Esther. I think you’re part of the way there but there’s a bit more detail that could be added to provide a more complete explanation.
Atrial flutter (300 bpm) with a Wenkebach effect
Atrial flutter with multilevel AV nodal block. The atrial rate is approximately 300bpm. There is variable AV conduction going on and the AFL-R wave appears to increase until there is a dropped beat. However do not think this is classic Wenckebach type pattern as there aren’t two consecutive flutter waves that conduct, therefore it looks like multilevel / dual AV nodal block involving the upper and lower AV node. I can see there are beats of slightly different QRS morphology every 1st and 3rd beat in the pattern which doesn’t follow Ashmans Phenomena, it might just be respiratory variation.
Great analysis, Kathryn. I’ll construct a laddergram within the next few days to show exactly what I think is happening.
Flutter auricular con bloqueo 2.1 alernando con bloqueo 4,1