Dr Dave Richley

Answer Added 31.07.24
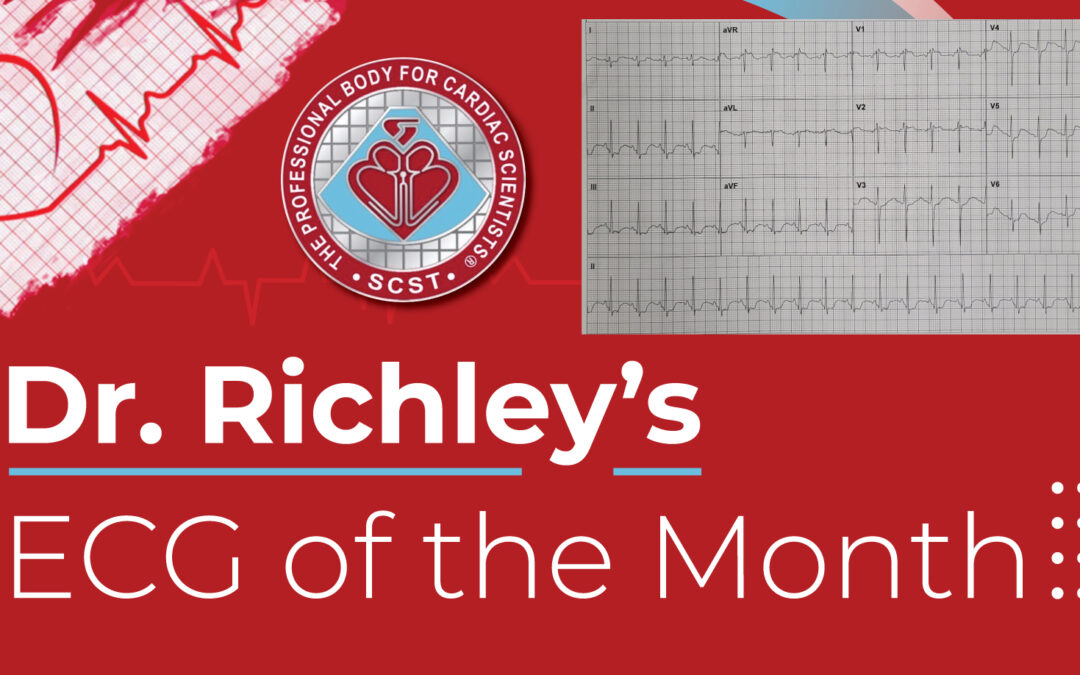
What does the ECG show? There is sinus tachycardia with a heart rate of 115 bpm and a borderline right axis deviation of +90 degrees. There is ST depression in leads II, III and aVF and V3-V6. Additionally, there are rSr’ complexes and ST elevation in V1 and V2. There is also a big U wave, partially merged with the T wave, in several leads, perhaps most noticeably in in V3-V6, and in V3 the U wave is taller than the T wave.
Many people, when they see ST depression, automatically assume that it is due to myocardial ischaemia, but ST depression has a number of possible causes, including hypokalaemia.
It is well known that tall U waves are typical of hypokalaemia but often big U waves, because they are fused with the T waves, are not recognised and it is mistakenly thought instead that the T waves are abnormally large, producing a prolonged QT interval. In several leads here, though – such as from V4 to V6 – the twin peaks of the T and U waves can be clearly seen.
What about the unusual appearances in V1 and V2? Perhaps the ST elevation is a reciprocal manifestation of the ST depression in V6, or maybe it indicates a type 2 Brugada pattern. The small amplitude of the 2nd r wave and the rapid descent of this deflection are more in keeping with ‘incomplete right bundle branch block’ than Brugada syndrome. Sometimes this pattern is produced by siting the V1 and V2 electrodes too high, and the negative P waves here support that explanation.
To conclude, this ECG shows features of hypokalaemia – which was subsequently confirmed – and ST elevation and an rSr’ pattern in V1 and V2, which may be due to a combination of reciprocal changes and high placement of the V1 and V2 electrodes.
Many thanks to the contributors who posted their invaluable observations and reasoning.
There is fairly widespread ST depression and abnormal T waves which I think are possibly being extended by U waves (lead l shows a dip after the T and rise again for the start of the U). Both of these findings are suggestive of hypokalaemia, which also correlates with the patient’s history. I also think that there is a Brugada type 1 pattern in V1 and V2, which may have been unmasked by the hypokalaemia?
Thanks very much, Beth. I won’t comment just yet.
Brugada type 2 with a saddleback shaped ST elevation in V1 and V2
Thanks, Emma. That’s an interesting observation, which I’ll discuss when I post my explanation.
Pathological increase in U-waves indicates hypokalemia. There is an r-wave at the end of lead V1, which may be due to the placement of the V1 lead electrode too high. Because the p-wave of V1 is completely negative.
Thanks, wck – astute observations and good reasoning.