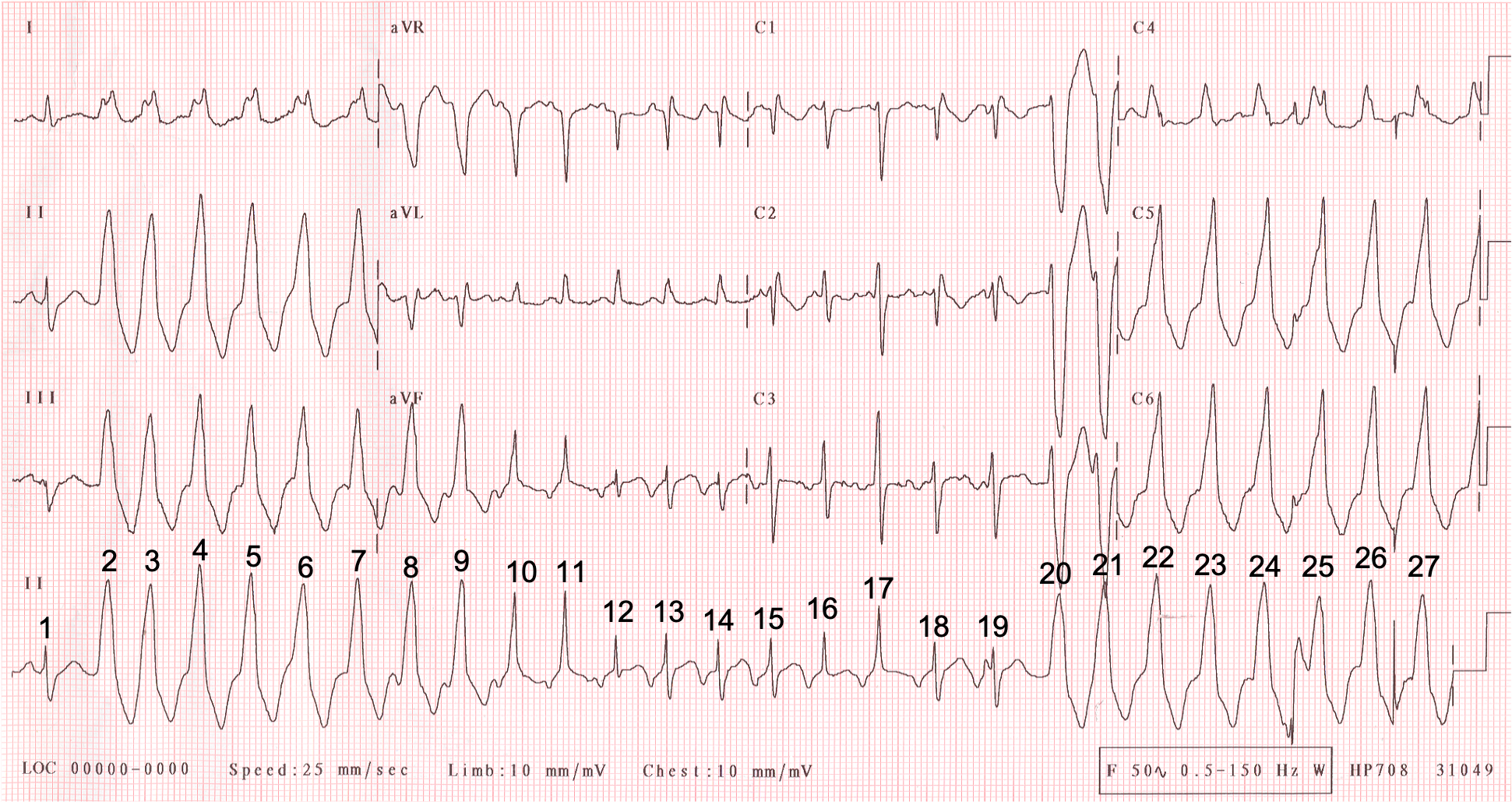
This month’s ECG is one that I’ve had in my collection for many years, filed under ‘Don’t know’. I do have a possible explanation for what’s going on here but I’m far from certain that it is right, so I’d welcome your ideas and suggestions. Unfortunately, I don’t have any clinical information. I have numbered all the beats to facilitate the discussion. Please let me know what you think.
Dr Dave Richley
Initial thought was AF with pre-excitation but that’s too obvious…
I was the same, AF with aberrance..
Thanks Mags. Definitely worth considering but I don’t think it’s the answer.
SVT with aberrancy offset by PVC
Possible brugada syndrome seen in v1,v2
Thanks, Ramadan. I initially wondered about aberrancy but how could that explain the continually changing QRS morphology in the middle of the tracing? Tricky. Also, I don’t think it’s typical of Brugada, but I may be wrong.
Polymorphic VT with Atrial Ectopics?
Thanks, Sophie. Polymorphic VT certainly has to be considered when there is a regular tachycardia with continually changing QRS morphology, but how would you explain the narrow complexes? And which beats do you think are atrial ectopics?
As always, an intriguing and challenging case, Dave! Probably worth sharing on Twitter at some point.
I think this is a rare case of two different arrhythmias occurring simultaneously — one supraventricular and the other ventricular.
1. R1 = sinus beat, or at least it seems that way.
2. R2-7 = R20-24 = R26-27 = non-fused beats of RVOT VT, not “LBBB” aberrancy”, as suggested by the LBBB morphology, R/S transition at V3/4, and prominent inferior axis.
**I think the WCT is a tad irregular — not entirely strange for VTs
3. R8-11 = varying degrees of fusion between the SVT and the VT
4. R12 = possibly the only beat of the SVT that is non-fused, or at least non-aberrant
5. R13-15 = R18-19 = non-fused beats of the SVT, which is a long R-P tachy, with inverted P waves in the inferior leads, upright in aVR and V1, and ?biphasic in V3. I believe this to be an AT (with RBBB aberrancy, as seen in V1) from possibly low in the RA. Of course, it could also be an atypical AVNRT or orthodromic AVRT (with RBBB aberrancy), but I think an orthodromic AVRT is unlikely.
**If we go backwards, from R19, we can see the P waves “march through” and then disappear into the WCT — I believe this signals that both arrhythmias co-exist. We know that AVNRTs can march on undisturbed by PVCs if they are His-refractory — no reason why short runs of VT would be any different. ATs also tend to be walled off from the influences from the ventricles. It does not seem like the SVT continues after 19, or at least, it is difficult to tell. I can not see any obvious evidence of atrial activity beyond that point, as we see between R8 and R11.
I am by no means certain. It’ll be interesting to read other thoughts on the matter.
Great comments, Ōkóyè Ō – thanks very much. I think we’re about 90% in agreement but of course it may be you that is correct where we differ. I’ll post my explanation and laddergram in a day or 2 and invite further comment.