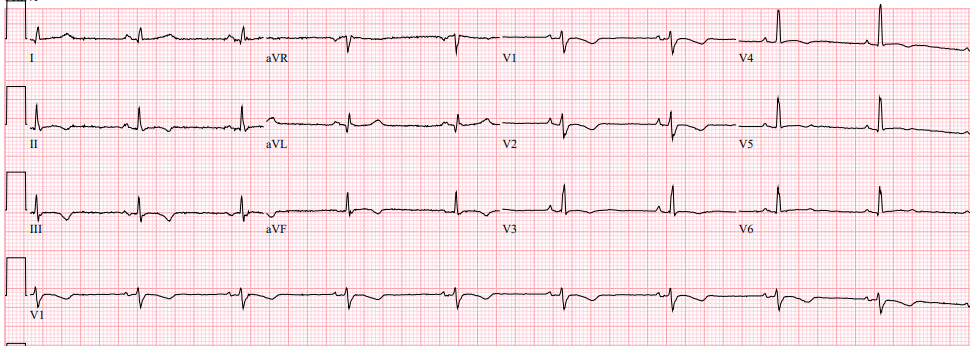
This ECG was recorded from a 40-year old male who was resuscitated from a cardiac arrest while playing football. There was no medical history of note except that he had recently noticed that he was getting more breathless on exertion.
What abnormalities are present and what clinical diagnosis is suggested by them?
Dr Dave Richley,
Associate Lecturer
Newcastle University
Its a cardiac ischemia
Ischaemia.Widespread t wave inversion
Is it Brugada
Thanks to Monay, Karen and Becky for their responses.
Monay and Karen suggest myocardial ischaemia as the diagnosis, but while ischaemia certainly can produce ST depression and should always be considered as the possible cause of a cardiac arrest, T wave inversion has very many possible causes – it is the most non-specific of all ECG abnormalities. So, is there anything else on the ECG that can help to narrow the range of diagnostic possibilities?
Becky asks if this can be a Brugada. Brugada syndrome is a known cause of cardiac arrest and is often associated with T wave inversion in V1, but the widespread T wave inversion we see here and the lack of the distinct pattern of ‘coved’ ST elevation in V1 and V2 that characterises the condition argue against Brugada syndrome in this case.
Sinus bradycardia
Normal QRS axis
Normal intervals including QT (not measured) – visually looks normal
Widespread T Wave inversion – flattened/biphasic V5-V6
No obvious epsilon wave which could indicate RV conduction delay in ARVC (in 50% of patients with ARVC)
BUT…
There could there be ‘prolonged S-wave upstroke in V1 and V2 with ? localised QRS widening’ – Another possible feature of ARVC
Excellent observation and deduction from Joe Shipton. This was indeed a case of arrhythmogenic right ventricular cardiomyopathy. As Joe points out, there are no epsilon waves but the prolonged and ‘jerky’ upstroke of the S wave in V1 and V2 has the same significance as epsilon waves, indicating delayed activation of diseased regions of the right ventricle. This is a subtle but important feature of the ECG, and I will try to get a close-up picture of it uploaded later. The T waves are markedly inverted in V1 and V2, the chest leads closest to the RV, but the T wave inversion is really quite extensive and this is most likely due to left ventricular involvement: in most cases of ARVC, although the initial manifestations of the disease may be due to of its effect on the right ventricle, the left ventricle is also affected. ARVC is one of the commonest causes of sudden death on exercise in young adults.