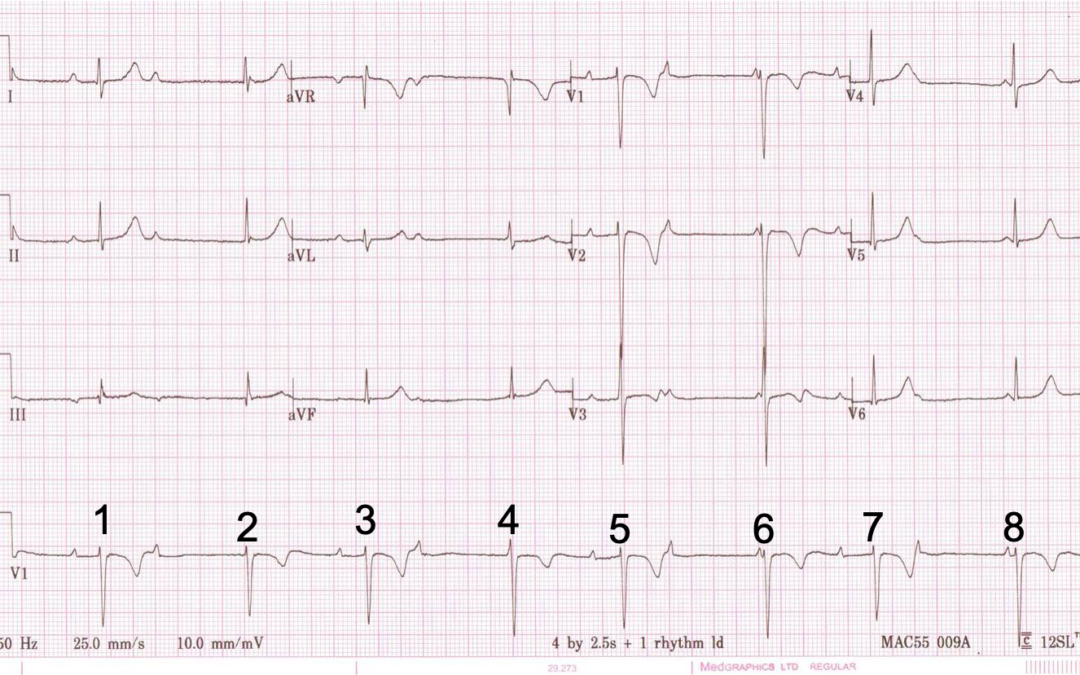
I don’t have any clinical history to go with this ECG, but how best should we describe the rhythm? I have numbered the beats to facilitate discussion.
Analysis & continuing discussion below
I agree with Scott’s analysis that this is second-degree AV block in which beats 1, 3, 5 and 7 are conducted beats and beats 2, 4, 6 and 8 are junctional escapes. There is an underlying sinus arrhythmia in which two of the P waves cannot be visualised because they occur simultaneously with QRS complexes (beats 2 and 4).
Once all the P waves have been identified it can be seen that only 1 in 3 of them are conducted. This may lead some to describe this as an example of high-grade block, but only one of each pair of non-conducted P waves can truly be described as being blocked – failing to conduct when they would be expected to – because the other non-conducted P wave in each pair occurs at such a time – almost simultaneous with the junctional discharge – that it cannot possibly conduct to the ventricles.
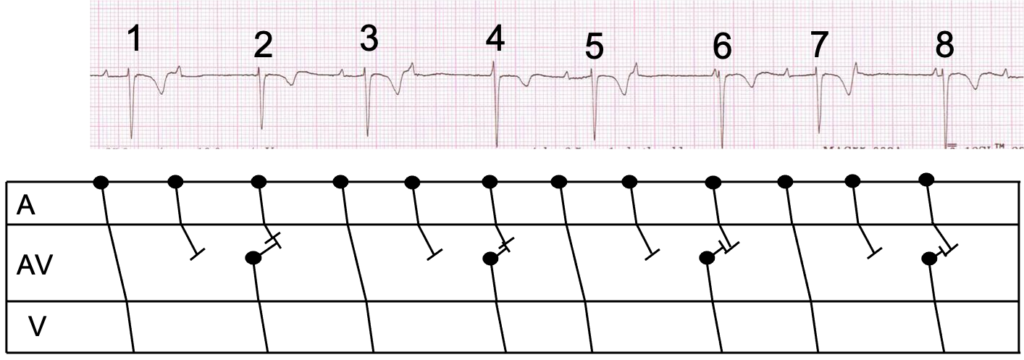
As there are never two consecutively conducted P waves, this cannot be described as either Mobitz I or Mobitz II AV block. Instead, it is a variety of second degree block that doesn’t fit comfortably into the Mobitz classification. The phenomenon we see here in which conducted beats alternate with escape beats is often described as an escape-capture bigeminy. I have tried to illustrate all of this with a laddergram, which now accompanies the 12-lead ECG.
One question: why do the PR intervals of the conducted beats vary slightly?
Continue the discussion in the comments and share your thoughts.
The question I asked above is: why do the PR intervals of the conducted beats vary slightly? The answer is linked to the sinus arrhythmia. The refractoriness of the AV node, and therefore its ability to conduct, depends on the time that elapses between an escape beat and the next P wave, which is assessed by the RP interval – the time between the beginning of the QRS and the beginning of the next P wave. The longer the RP interval, the longer the AV node has to recover and the better it can conduct. A long RP interval is therefore associated with a short PR interval and vice versa. This is known as RP/PR reciprocity and it is clearly demonstrated by comparing beats 3 and 7 – see below. The RP interval to beat 3 is 840 ms and the PR interval of beat 3 is 260 ms. Because of the sinus arrhythmia, the RP interval to beat 7 is only 660 ms and the PR interval consequently increases to 320 ms.

Dr Dave Richley,
Associate Lecturer
Newcastle University
I get the feeling this would be Wenckebach, but gets complicated by relatively early junctional escape complexes, ventriculophasic sinus arrhythmia, and possibly atrial ectopy.
The atrial rate remains ~75bpm, with variability of the P-P interval and P-wave morphology, which depending on the patient could be physiological (phasic respiration/ventriculophasic sinus arrhythmia), or pathophysiological (atrial ectopy).
The R-waves which appear to be conducted have PR intervals 240ms(1) to 320ms(7) – as the overall sinus rate very slightly increases. The R-P interval of these R-waves is not consistent enough to suggest re-entrant atrial echo beats. The non-conducted P-waves following 5 and 7 have a slightly more peaked morphology, although this may be a red herring, and due to respiration rather than a change in focus.
Junctional R-waves 2 and 4 almost entirely mask the concurrent P-waves – which for complex 1 is visible in lead 1 at the end of the QRS. The overall sinus rate then increases slightly unmasking them for 6 and 8.
The P-P intervals successively accelerate in cycles of 3 following each non-conducted P-wave, which i believe represents the ventriculophasic response.
In conclusion, I think this is variable 2nd degree AVB with a relatively fast junctional escape rate, and ventriculophasic sinus arrhythmia – although it could be CHB with junctional escape and concurrent junctional bigeminy; as always, a longer recording of this rhythm would reveal the true relationship between atrial and ventricular activity.
Good ECG!!!
Perceptive comments, as always , Scott. Just for complete clarity, which beats do you think are conducted and which do you think are junctional escapes?
The odds are conducted (1,3,5,7), with the remainder being escape complexes, probably.
I interpret this ECG as an AVD rhythm.
The slight variations in PP intervals are due to ventriculophasic phenomena. The PP intervals about 3.6 and 4.0 small boxes. Otherwise it is quite regular.
The QRS of 2, 4, 6 & 8 are junctional rhythm (escape).
The QRS of 1, 3, 5 & 7 are (normally) conducted impulse, hence they are captured atrial beats.
Hence I would interpret this case as having AVN conduction disease.
Conclusion:
The ECG demonstrate an atrial rate of between 75-80/min with AVD and slow junctional escape rhythm with escape-capture bigeminy.
Not having any history makes it difficult and its a little tricky ECG.
Could it be…………
Underlying sinus with 1st degree AVB (beats 1, 3, 5) with non conducted PAC’s (slight P wave morphology change) leading to post extrasystolic pause and Junctional escape beats (2, 4 6 and 8)
Beat 7 is a slightly prolonged 1st degree sinus beat ( I say this as the T wave inversion is the same depth as the beats I have called “sinus” and slightly shallower in the “junctional” beats.
Beats 6 and 8 being junctional and coincidently occurring with atrial activation as the timing slightly changes
And what are peoples thoughts on the the T wave inversion in V1 – V3?
Thanks for the comments, Glenn. I don’t think these are non-conducted atrial premature beats because the atrial rate is only slightly irregular and the variation in P wave morphology is very minor. I think sinus arrhythmia with 2nd degree AV block is more likely, although I can’t be certain. I agree with Scott Walton – see below – that the T wave inversion is probably age-related: the T wave shape as well as polarity, together with the sinus arrhythmia, suggests that the patient is young.
This ECG is probably from a younger patient, so is possibly vagally mediated nodal AV block, and would contribute to sinus arrhythmia, variable T-wave amplitude, and variable PR interval, with phasic changes occurring with respiration during the recording. This could also account for the T-wave inversion in V1 – V3.
Thanks for all the info