I don’t have any clinical information in relation to this month’s ECG, but what I’m interested in is the rhythm and conduction. I don’t think it’s quite as straightforward as it first appears and I’m not absolutely sure of everything that’s going on.
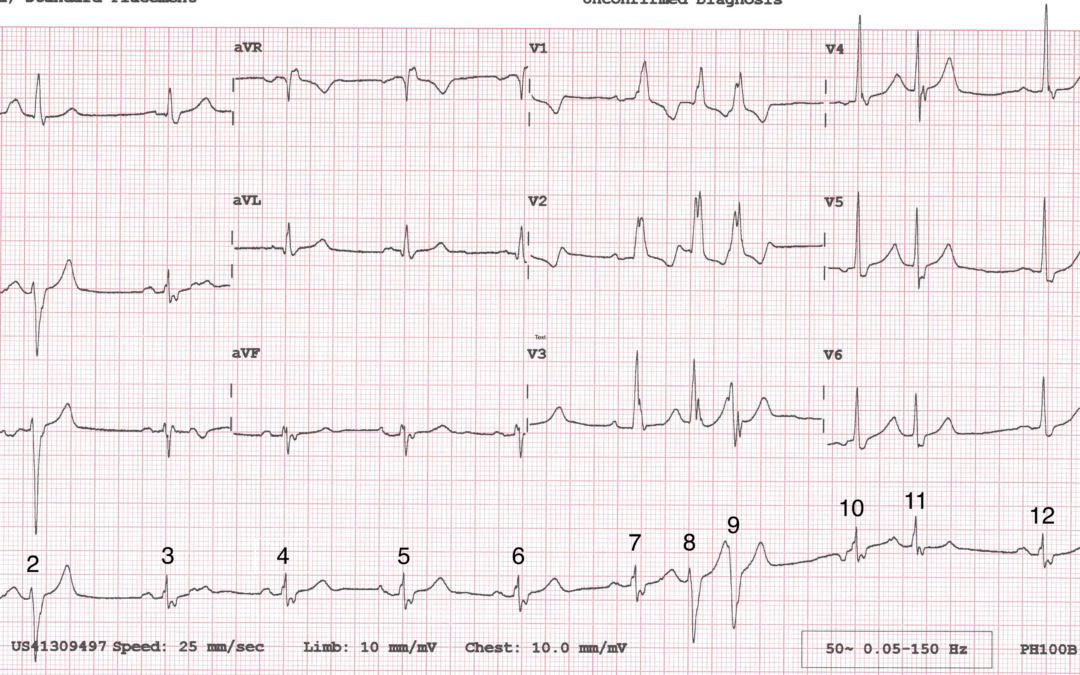
I’ve numbered the beats to facilitate discussion and I’d be very interested to hear people’s thoughts.
Dr Dave Richley,
Associate Lecturer
Newcastle University
The rhythm is Sinus rhythm. QRS morphology is widened suggestive of Bundle branch block (in this case RBBB). The premature beats could be supraventricular with aberrancy due to the change in morphology but NOT axis.
Starting with the P waves I can see at least 3 morphologies, beats 4, 5 and 10 all have different P waves but similar PR interval and QRS morphology- based on this I think I could call it a wandering atrial pacemaker.
Beat 3 is followed by a non-conducted early P wave which is seen as a notch in the T wave. Beat 1 has an early p wave hidden in the T wave as well but this one does conduct and I think it conducts aberrantly. I also think beat 8 is the same as beat 2 (an aberrantly conducted atrial beat), and beat 9 could be an R on T but it’s suspicious that it’s such a similar morphology to beats 2 and 8.
Overall given the various P wave morphologies and differing P-P intervals I think there’s evidence to call it wandering atrial pacemaker and the different QRS morphologies we see are likely due to aberrant conduction as some of the ventricle are still in the refractory period. But I couldn’t rule out an R on T for beat 9 and can’t see a clear P wave preceding it.
Thanks for your comments. Leah. I agree with you about the aberrantly and the non-conducted atrial premature beats, but I don’t think I would describe the rhythm as being due to a wandering atrial pacemaker. I think of it as SR with frequent APBs and maybe 1 atrial escape beat. I’m glad you pointed out the differently shaped P wave before beat 5 – I’m not sure whether this indicates a beat of atrial origin or whether there is an artefact that’s distorting a normal P wave, but I am tending to agree with you that it indicates an atrial origin.
Thanks to Kamile for the comments. I agree that the QRS morphology does suggest RBBB, although the pattern is not quite typical. Kamile says the premature beats could be supraventricular in origin, but is there any way to be certain? And are there any other rhythm abnormalities?
SR, RBBB, leftward axis. Atrial ectopics with a more leftward axis indicating likely bifascicular block with left anterior hemi-block. P-wave for complex 2 is clear in lead III, still visible in lead II. The same P-wave is just perceivable in lead II preceding complex 8 which displays the same intraventricular conduction pattern, meaning there is likely a more hidden P-wave preceding QRS 9.
The nonconducted P-wave in the ST segment of complex 3 is much more obvious, although fails to interrupt the sinus rate for reasons unclear*.
Complex 10 displays an inverted P-wave, indicating probable atrial escape, which again fails to interrupt the next sinus P-wave, and may represent some form of retrograde SA block*.
There may of course be something deeper and more meaningful that I’m missing here?
Hi Dave. Ok I’ll give this a shot. Initial thoughts. As far as I can see beats 1, 3, 4, 5, 6, 7 and 12 are sinus beats (QRS preceded by an upright P wave in lead II). These sinus beats appear to indicate RBBB (rSR in V1 and S waves in leads I and V6) so I’m a bit confused as to why this isn’t “typical” RBBB as per your comment above. The sinus beats appear to have a normal to physiological left axis (within normal range). The premature beats are 2, 8 9, and 11 and also appear to have a RBBB morphology but the axis shifts to abnormal left > -30 degrees (best seen in lead II). So, I think these are either ventricular premature beats or atrial premature beats (RBBB with additional left anterior fascicular block). Having seen Scott’s comment, I think is probably the latter as missed the abnormal P wave preceding beat 2 in lead III. What’s bugging me is the P wave before beat 10 (which is inverted) and a possible P wave after QRS 3 (which Scott also mentions, and I initially thought was artefact) so I can’t exactly work out exactly what’s going on here 🙂
Great comments from Scott, with which I almost completely agree.
The premature beats are of atrial origin, as evidenced by the fact that they’re preceded by premature P waves. They are conducted with left anterior fascicular block aberrancy as well as the RBBB shown by the sinus beats.
Scott spotted the non-conducted atrial premature beat immediately after complex 3, but like me he doesn’t understand why it doesn’t interrupt the sinus rhythm: normally a premature atrial impulse will depolarise the sinus node, re-setting it and delaying the appearance of the next sinus beat. We don’t see that here.
Scott also points out the inverted P wave before beat 10, suggesting that it represents an atrial escape beat, although it occurs after an unusually short pause. I suspect that beat 11 is an atrial premature beat rather the next sinus beat, and it appears to be conducted with a slight degree of aberrancy – the QRS morphologies in beats V4, V5 and V6 are different from those of the sinus beats.
Max has some similar thoughts, and like me is puzzled by the inverted P wave before beat 10. She asks why I think the RBBB is not typical. Maybe I’m being picky (it wouldn’t be the first time) but RBBB is characterised by an rSR’ or QR pattern in V1 with a broad, tall terminal R wave. Here, however, there is no S or Q wave, which means that in V1 (and V2/V3) there is instead a single broad, notched R wave, which strictly speaking is not typical of RBBB.
So, I think the remaining questions are: why is there no incomplete compensatory pause after the non-conducted APB following beat 3, why does an atrial escape beat appear only a short pause after the pair of APBs (beats 8 and 9), and is beat 11 a sinus beat, as Scott suggests, or an APB, as I suspect?
Any additional comments or alternative explanations would be very welcome.
Hi Dave thank you, Just putting this out there. Although I can see that beat 2 is an APB, can we be absolutely certain that beats 8 and 9 are APBs and not VPBs?
Hi Max – if you look very closely, you may just be able to make out a tiny deflection on the ascending limb of the T wave of beat 7. I think this is a premature P wave. Also, the QRS morphology of beat 8 is very similar to that of beat 2. I can’t prove that beat 9 is also an APB but again the QRS is similar and I do believe there is a tiny deflection, maybe representing a premature P wave, immediately after QRS 8 in V3. A phone may not be ideal for seeing these details!
As the rate is almost exactly 60bpm, atrial pacing would explain the lack of non-compensatory pause. I can’t make out any spikes no matter how zoomed in I get, but this would be a rational explanation based of AAI or DDD atrial refractory period.
It could also be His bundle pacing with non-selective capture causing the RBBB pattern, with premature atrial beats above upper tracking rate.
This is the problem with a lack of relevant clinical history.
Interesting idea – I hadn’t thought of the possibility of pacing. I’ve returned to the original I was sent and I just can’t see any evidence of pacing spikes. Also, wouldn’t beat 3 have appeared a bit earlier if it had been paced?
That looks like it’s from a Philips ECG machine, there should be a P or P? At the very bottom right hand corner (it’s just about cut off on this scan) that indicates whether the Pacing filter is on, it may be worth knowing that
Basic rate 60ppm, hysteresis 55ppm. I really can’t see pacing spikes either, which is possible with very low pacing output (1V) combined with low pass ECG filtering.
I’mpretty sure this isn’t the case, it’s just so suspiciously 60bpm for the regular rhythm and would explain the lack of non-compensatory pause.
#Clutching at straws
Maybe not so much clutching at straws as exploring every possibility, Scott. I’m wondering whether there is intermittent sinus node entrance block, such that the sinus node is sometimes protected from depolarisation when there is an atrial premature beat, and I think this is what you may have been alluding to in your original comment. However, I don’t know if this phenomenon even exists!
https://www.ajconline.org/article/S0002-9149(01)01624-1/fulltext
I don’t have access though.
I’ve certainly seen interpolation of junctional ectopics, more likely a representation of simultaneous conduction via dual AV nodal pathways.
Yes, I did call it possible retrograde SA block, which is the most fitting description I could come up with.
Thanks for the link – very interesting. One of the references in the paper documents the existence of sinus node entrance block, so it is a real phenomenon. Maybe we’ve just about got to the bottom of this one now?https://www.ahajournals.org/doi/pdf/10.1161/01.CIR.44.5.789