Once again, I don’t have any clinical information but how would you describe and interpret this ECG? It’s probably unreasonable for you to be expected to make a definite diagnosis but based on what you can see, what are the most likely possibilities?
The Answer
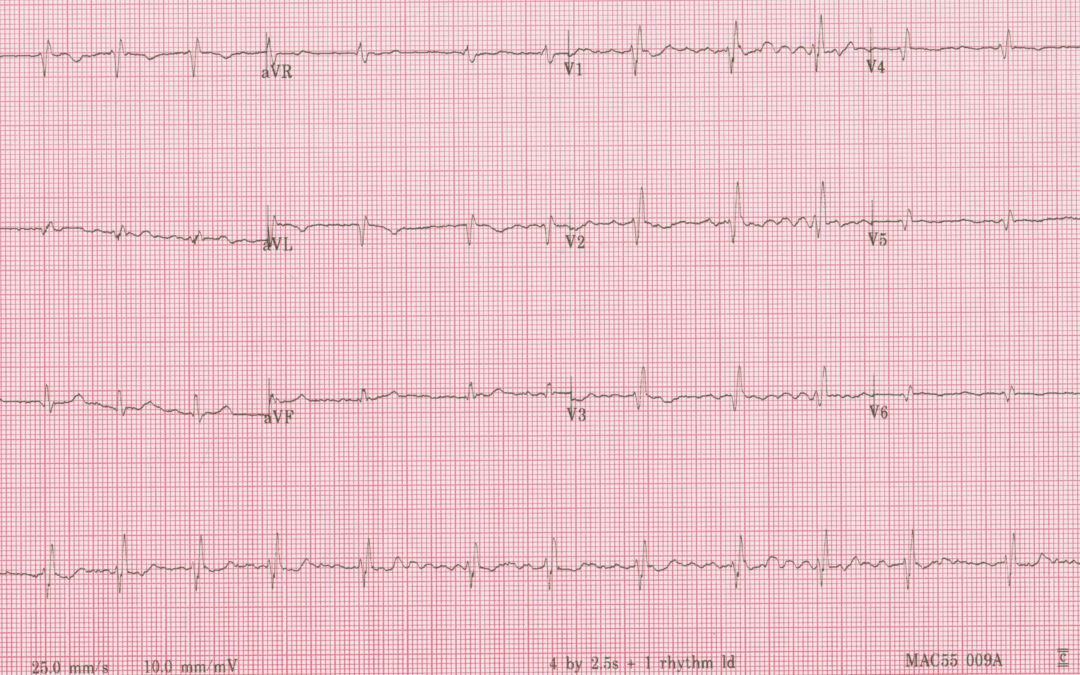
This time, for a change, we’ll start with the conclusion. This is an example of mirror-image dextrocardia, as several of you suspected, but’s it’s not an obvious, straightforward case to diagnose because in addition there is atrial fibrillation and right bundle branch block.
Dextrocardia is usually recognised electrocardiographically by all the deflections in lead I being negative and all the chest lead QRS complexes being negative with diminishing amplitude towards V6. In this case, because the rhythm is atrial fibrillation, there are no negative P waves in lead I to support a suspicion of dextrocardia. Yes, the QRS is negative in lead I but this can have a number of causes including right ventricular hypertrophy, left posterior fascicular block, swapped left arm and right arm connections and lateral myocardial infarction. When we turn to the chest leads to help us, we find that although the QRS complexes show diminishing amplitude from V2 to V6, there is not a persisting negativity; in fact, all the chest leads show predominantly positive complexes.
The complicating factor here, of course, is the right bundle branch block (RBBB). The characteristic ECG appearances in RBBB are due primarily to delayed and prolonged depolarisation of the right ventricle (RV): initially, ventricular depolarisation is normal, with left-to-right activation of the septum and rapid activation of the left ventricle, but then the ECG shows a broad terminal deflection due to RV depolarisation. In mirror-image dextrocardia, the morphological RV (the one that has a moderator band and receives deoxygenated blood which it pumps up to the lungs) is of course on the left. This means that initial septal activation takes place from right to left, producing an initial small R wave in all the chest leads, which are all to the left of the ventricles. There is then depolarisation of the rest of the LV, which of course is on the right in dextrocardia, and this produces an S wave in all the chest leads. Note that this S wave gets smaller from V1 to V6, as the chest electrodes get further and further from the morphological LV. There is then the delayed and prolonged depolarisation of the morphological RV, which proceeds towards the left, producing a broad terminal R wave from V1 to V6 that diminishes in amplitude as the chest electrodes become progressively remote from the RV.
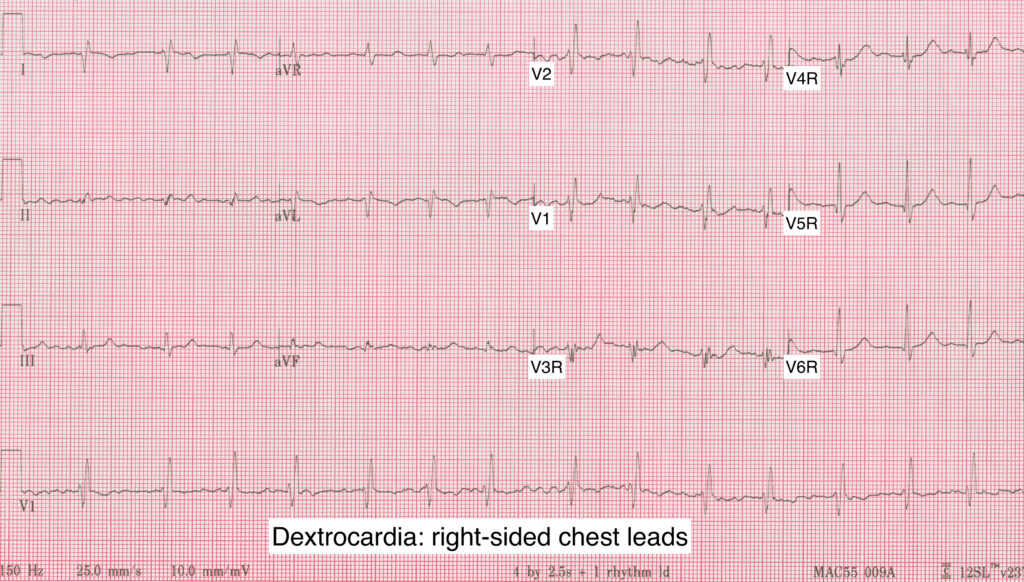
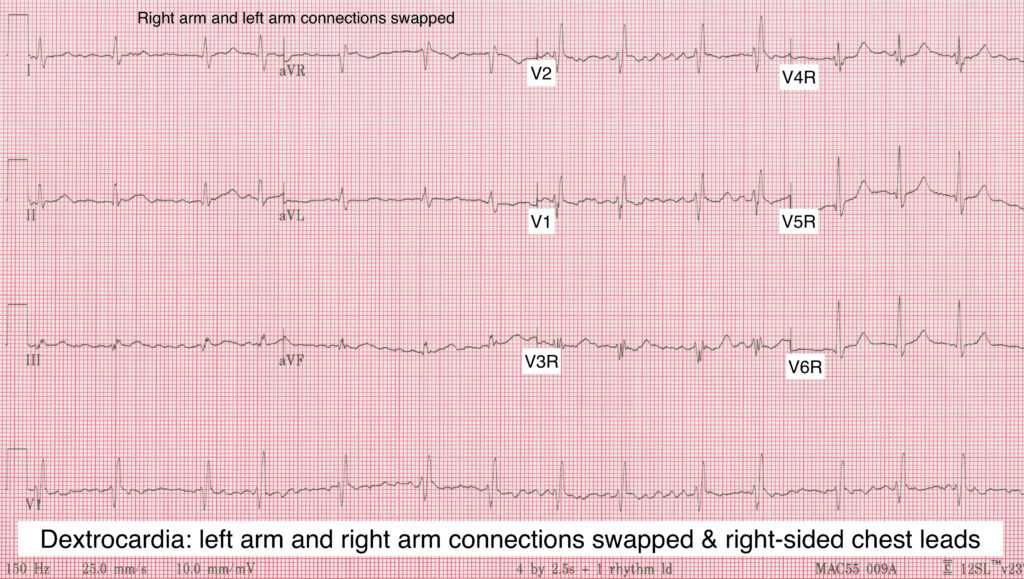
This ECG is therefore completely consistent with mirror-image dextrocardia, and just to prove it here are two repeat recordings, one with right sided chest leads and one with swapped right arm and left oarm connections in addition to right sided chest leads.
I am very grateful to Kate Hardy, PTP student at the University of Sunderland, for sharing these ECGs with me.
Well my first thought was that the right and left arm leads had been transposed but in the absence of ‘p’ waves due to AF that made it tricky to confirm but the low voltages in V4-V-6 might be suggestive that if the R and L arm leads weren’t transposed then it could be dextrocardia with AF. Partial RB3 also a bit suggestive of congenital component in the context of dextrocardia.
Absence of calibration signal could throw cat amongst pigeons re voltage criteria if someone had tinkered with the standardisation settings. In summary – glad it’s not my ECG.
Mags- my first thought was also a transposition of leads or incorrect placement but dextrocardia could be the explanation if the ECG placement is correct. We have the same ECG machines at our hospital, it is set to 10mm/mV, it will say 10/5 if the chest lead gain was changed.
Great comments, Mags and Katy. I’ll refrain from saying any more at this point.
There is atrial fibrillation with a normal ventricular rate. The QRS axis is approx.+150 degrees (abnormal right axis). There is dominant R wave in V1-V4. QRS duration appears slightly prolonged in V1-V4. Has a RBBB pattern but it’s definitely not a typical RBBB (lack of S waves in lateral leads). Voltages appear low in some of the inferior leads and they appear to diminish from V1-V6. T waves are either flat or negative in a lot of the leads. I think there are pathological Q waves in leads I and aVL, and V4-V6. Not 100% sure about Q waves in V1-V3 (can’t tell whether there is a really small initial R wave or whether it’s a fibrillation wave).
I can see why people say that this might be dextrocardia (negative lead I, right axis, and diminishing voltages in the chest leads), but without a negative P wave in lead I, I’m not convinced. There are indications that there could be right heart pathology (ASD, RVH etc) but again not totally convinced. The AF makes me think this is an ECG of an older person. I could be wrong, but I personally think the Q waves might be a clue as to the cause of the changes we see here. Thanks Dave!
Bloqueo de rama derecha y fibrilación auricular
With how regular the R-R interval is (and P waves preceding them?) I suspect beats 2-4 and 7 may be sinus, but the rest very much feels like Atrial Fibrillation.
RBBB morphology and right axis deviation present with similar QRS morphology.
With I being inverted and aVL and aVR being swapped it initially seemed like a Left-Right arm swap. I won’t pretend I thought of Dextrocardia until the other comments mentioned it, but the falling QRS amplitude and with II being more isoelectric also I think that would fit pretty well.
Having said all that, I hadn’t considered it before but in dextrocardia the bundle branches would also be mirrored, so would that make this a LBBB? (Assuming the bundle branches are named for fasicular anatomy not the side of the body they’re on)
I think I’ve just started confusing myself about which bundle is blocked!
I’m not 100% sure that this is dextrocardia, but that’s a really good question. Never seen a dextrocardia with bundle branch block. I tried to look for one online but they seem to be rare cases behind a paywall. You’re right, the bundle branches go with the ventricles so they would be swapped over but I don’t think it’s as straightforward to say that the normal RBBB and LBBB ECG patterns would be totally reversed.
You probably wouldn’t see the normal BBB patterns in the lateral leads but V1 (I imagine) would remain relatively unchanged in terms of predominant QRS direction in BBB. The way I see it is that V1 is sitting over the septum. The bulk of left ventricular depolarisation is still predominantly moving away from V1, whether the left ventricle is situated on the left or right side of the body. I assume then that if a patient has dextrocardia with LBBB, V1 would still be predominantly negative but broad. In RBBB, I think V1 would still be predominantly positive reflecting the wavefront moving back towards V1 to depolarise a left-sided RV. I really don’t know for sure. I’m probably assuming a lot. Also if there are other structural defects involved – then who knows what you would get. What do you think Dave?
Yes, it’s tricky isn’t it Max? Thanks for your detailed analysis. I’ll hang on a bit longer before I reveal the answer!
Thanks, Jon – good comments and an interesting question. Do others agree or disagree with the comments so far? Any new suggestions?
I have looked & looked at this ECG and can’t quite decide either.
I too thought possibility Dextrocardia with AF.
My other thoughts were…
Something is happening with the right heart.
So with the AF, maybe a PE? Which has dilated the right ventricle and shifted the axis.
Or they have a Dilated Cardiomyopathy which can result in Q waves in V1-V4..
both can result in RBBB.
Who knows, maybe it is just Dextrocardia! :’)
I had posted a comment but it seems to have disappeared? Apologies if this has duplicated.
Anyway.. I too thought this was Dextrocardia with AF, but then I thought, could it be that simple?
So, I did have some other thoughts..
It looks like there could be something occurring with the right heart.
So with the AF, maybe a PE? No S1Q3T3 but there is RAD & partial RBBB
PE may cause RV dilation but so could a dilated cardiomyopathy which could also explain the lack of precordial R wave.
But who knows, it could just be Dextrocardia, get them an Echo!
Thanks, Daisy. All good comments and I have to agree that this is not easy and straightforward.
I totally thought this was an old large lateral infarction. The initial R waves (representing septal depolarisation) are really tiny aren’t they? Or is it my eyesight? But good to see what a dextrocardia with BBB looks like. Such a good case – thanks for sharing Dave/Kate.
Yes, Max, the septal R waves in the chest leads are tiny – because of the distance of the chest electrodes in the standard positions from the heart. I have never seen this combination of abnormalities before either, and I’m not sure I would have worked it out with any confidence. Fortunately, Kate supplied me with the answer.
Hi Dave, can I please ask – the SCST guidelines document leaving V1 and V2 in standard positions, whereas the examples here have reversed V1 and V2 leads.
What’s the theory behind leaving V1 and V2 in standard positions? I ask because my (paediatric) department seems to do a bit of both and I want to standardise practice
Thanks!
That’s a very good question, Sian. The reason for the recommendation to leave the V1 and V2 in the original positions is that by swapping them round no new information would be provided, so there is no point – nothing is gained. The counter-argument, though, is that swapping the V1 and V2 electrodes would normalise the progression through the chest leads from left (V2) to right (V6R) and therefore make the modified ECG easier to interpret quickly. It could be argued that whatever is done, the most important action to take is labelling the recording accurately to describe where the electrodes were placed. SCST’s standards committee has just begun the process of reviewing the 2017 guidance on recording a 12—lead ECG and I have suggested to them that this review should include a re-assessment of the advice concerning electrode positioning in dextrocardia.