Here’s your December edition of Dr Richley’s ECG of the Month.
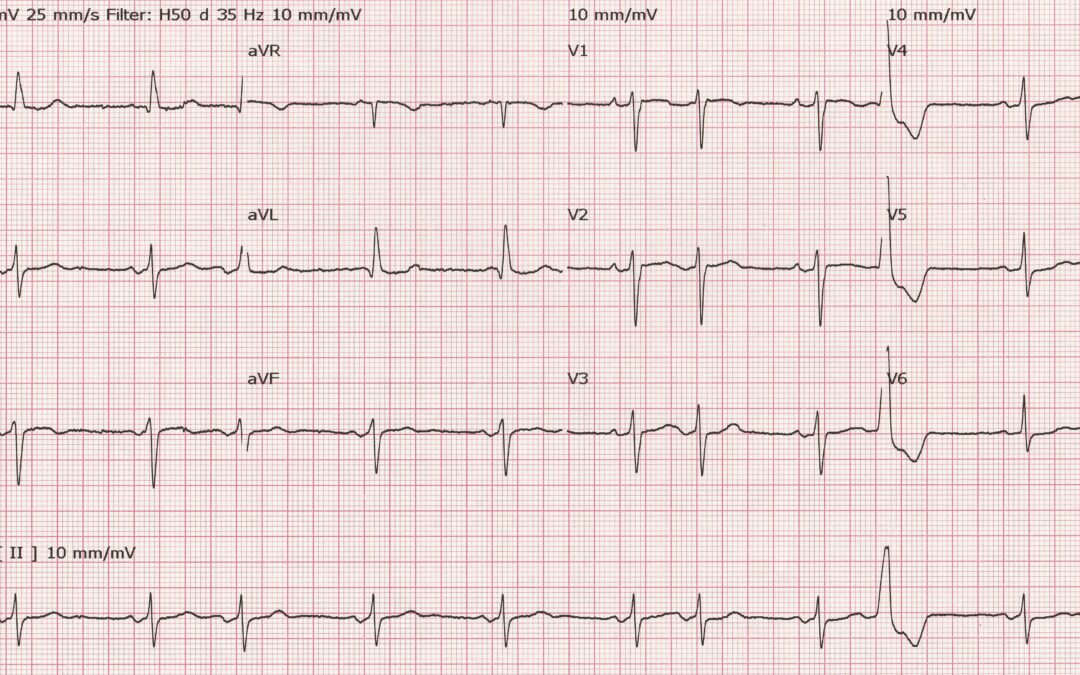
I came across this ECG recently and although I don’t know anything about the patient, I don’t think that’s vitally important for interpreting the tracing. I have to admit that it was the P waves that really caught my attention. So, how would you interpret this ECG?
Share your thoughts in the comments below and we’ll give you the answer later in the month.
The Answer
The most striking feature of this ECG is the abnormal shape of the P waves in leads II, III and aVF. These initially positive, then negative, P waves are typical of advanced interatrial block (IAB). Although first described in the 1940s and subsequently investigated in detail using various methods, including oesophageal electrocardiography, vectorcardiography and intracardiac electrophysiological mapping, IAB remains a largely unknown phenomenon.
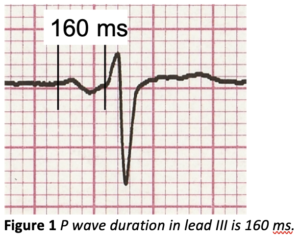
There is no agreed classification scheme and terminology for describing IAB but at its simplest IAB can be divided into partial and advanced block. In partial IAB, conduction in Bachmann’s bundle – a broad band of muscle fibres that connects the left and right atria high in the atrial septum – is delayed, leading to a widened, notched P wave, similar to that seen in left atrial enlargement. In advanced IAB, Bachmann’s bundle, owing to fibrosis, is not capable of conduction at all, so the sinus impulses must find a different route from right to left atrium. What happens is that the impulses are able to conduct from RA to LA by muscular connections in the region of the coronary sinus, low in the right atrium, then activate the LA in an upward and backward direction. The initial positivity of the P wave in the inferior leads is due to normal right atrial depolarisation; the terminal negative deflection is due to left atrial depolarisation proceeding in a very different direction to normal. In IAB, the P wave, as well as being biphasic, is prolonged to ³120 ms (1), as shown in figure 1 where the P wave duration in lead III in this month’s ECG is 160 ms.
 The negativity of the P waves in the inferior leads here might lead to a diagnosis of accelerated AV junctional, or low right atrial, rhythm but this would be mistaken. In an accelerated AV junctional rhythm in which the P wave precedes the QRS, the P wave is entirely negative, not biphasic, and the P wave negativity is seen in at least some of the chest leads, particularly V4-V6, as well as the inferior leads. Moreover, the P wave duration is not normally prolonged in accelerated AV junctional rhythm. For comparison, an example of accelerated AV junctional rhythm is shown in figure 2.
The negativity of the P waves in the inferior leads here might lead to a diagnosis of accelerated AV junctional, or low right atrial, rhythm but this would be mistaken. In an accelerated AV junctional rhythm in which the P wave precedes the QRS, the P wave is entirely negative, not biphasic, and the P wave negativity is seen in at least some of the chest leads, particularly V4-V6, as well as the inferior leads. Moreover, the P wave duration is not normally prolonged in accelerated AV junctional rhythm. For comparison, an example of accelerated AV junctional rhythm is shown in figure 2.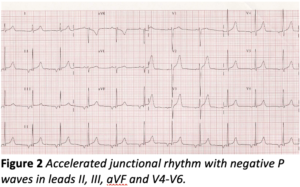
The clinical importance of advanced IAB is that it is associated with an increased probability of atrial arrhythmias such as atrial premature beats (as seen in this ECG), atrial flutter and especially atrial fibrillation (2). Moreover, advanced IAB is associated independently with an increased risk of transient ischaemic attacks (TIAs) and stroke (3,4). These associations have prompted speculation, and some research, on the possible benefits of antiarrhythmic drug therapy in patients with advanced IAB to prevent AF and anticoagulation to prevent TIAs and strokes, but so far the results have not been sufficiently persuasive to result in recommendations for prophylactic treatments.
Congratulations to Arron Pearce for recognising this unusual pattern.
- Bayés de Luna A, Baranchuk A, Robledo LAE, van Roessel AM, Martínez-Sellés M. Diagnosis of interatrial block. J Geriatr Cardiol 2017;14:161- doi: 10.11909/j.issn.1671-5411.2017.03.007
- Bayés de Luna A, Cladellas R, Oter R et al. Interatrial conduction block and retrograde activation of the left atrium and paroxysmal supraventricular tachyarrhythmia. Eur Heart J 1988;9(10):1112-8. doi:1093/oxfordjournals.eurheartj.a062407
- Ariyarajah V, Puri P, Apiyasawat S, Spodick DH.Interatrial block: a novel risk factor for embolic stroke? Ann Noninvasive Electrocardiol. 2007;12(1):15–20. doi: 1111/j.1542-474X.2007.00133.x
- Istolahti T, Eranti A, Huhtala H et al. The prevalence and prognostic significance of interatrial block in the general population. Ann Med 2020;52(3-4):63-73. doi: 1080/07853890.2020.1731759
The P wave axis doesn’t suggest sinus rhythm but a focus more to the left of the heart. I did wonder about a unknown case of dextrocardia but the R wave progression seems to rule that out
Thanks, Katie. Yes, you’re right that the chest lead R wave progression rules out dextrocardia. But can you explain why the P waves in the inferior leads start off positive, then go negative?
Delayed activation from left to right atrium.? Inferior leads have a biphasic appearance. Not quite sure on the short P-R interval in aVL.
Thanks, Claire – good see you here! You make an interesting suggestion but I won’t say any more for the moment.
Sinus bradycardia (only just) with 3 premature atrial ectopics and one premature ventricular ectopic. There is also 3rd degree inter-atrial block (advanced IAB) seen as biphasic P waves inferiorly. A sign of block within the Bachmann’s bundle. More common among very elderly patients. Only recently read about inter-atrial blocks so its fresh in my mind! I presume this is the main finding you wish to highlight on this ECG.
Thanks Arron – it’s great to see you joining the discussion. Interesting suggestions, but I won’t say any more for now.