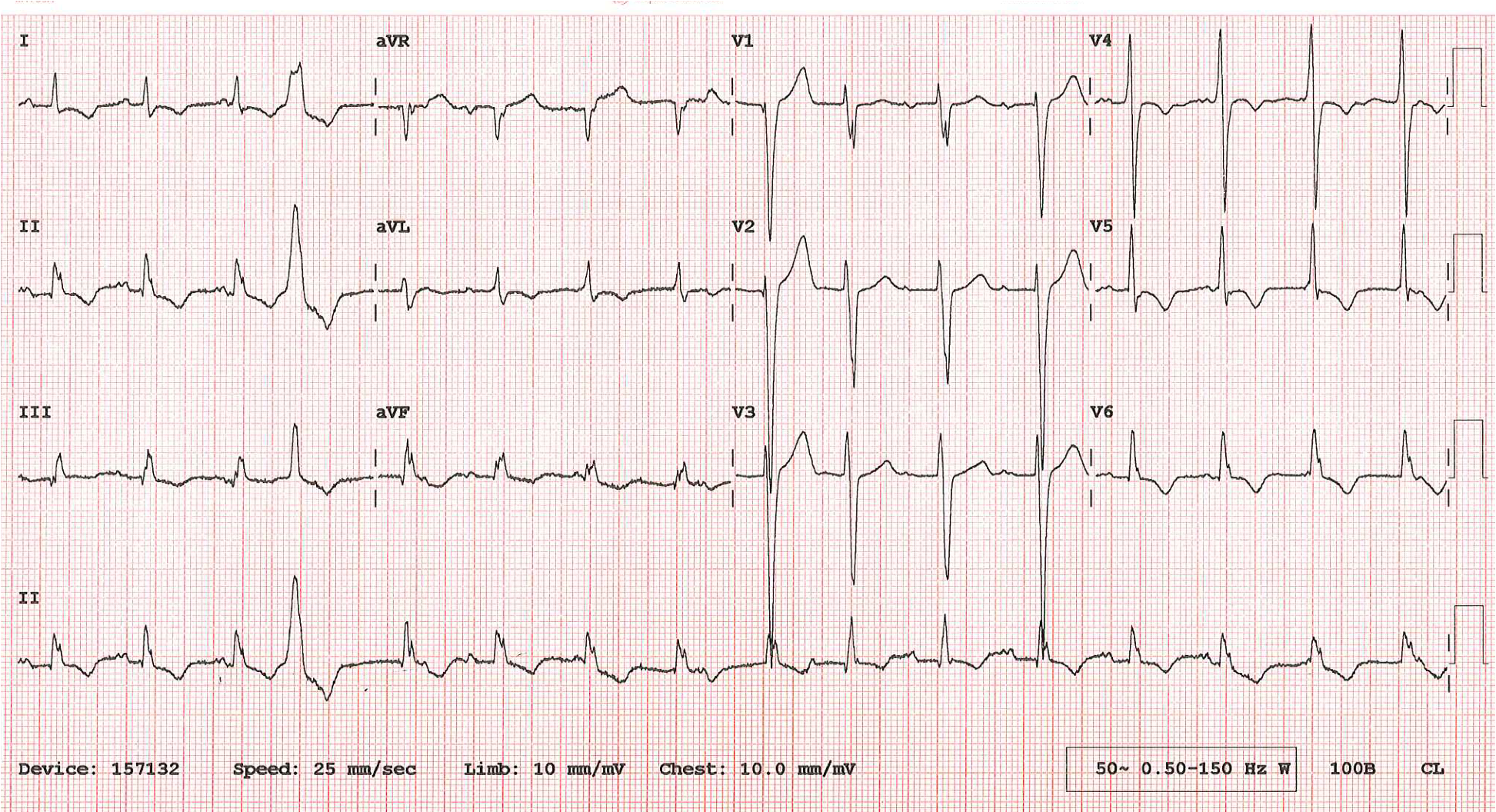
I was recently sent this ECG and asked what I thought the rhythm was. The ECG was recorded from a 55-year-old patient who had recently undergone aortic valve and root replacement following infective endocarditis.
I think I’ve worked out what’s going on but what do YOU think? Please provide as full an explanation as you can.
Thank you to Agnieszka Sawicka for supplying this months ECG.
The Answer
I have identified all the P waves with arrows and these show that there is an underlying sinus rhythm with an atrial rate of about 90 bpm. However, the ventricular rate is about 95 bpm and this is because there is an independent accelerated junctional rhythm. Very few of the sinus impulses are able to conduct to the ventricles, not because of any AV block but because in nearly every case they encounter an AV node that is in its refractory period and therefore incapable of excitation. This is a physiological rather than a pathological phenomenon.
There are two sinus impulses that, because of their timing, do manage to conduct and these are responsible for the two slightly differently shaped QRS complexes that I have labelled ‘S’. There is therefore incomplete AV dissociation.
There are also what appears to be one non-conducted atrial premature beat, labelled ‘A’, and one ventricular premature beat (VPB). The VPB probably conducts backwards part-way into the AV node, which blocks the next junctional impulse, causing the post-VPB pause, but not all the way back to the atria: I think the P wave immediately after the VPB represents a non-conducted sinus P wave rather than retrograde atrial activation.
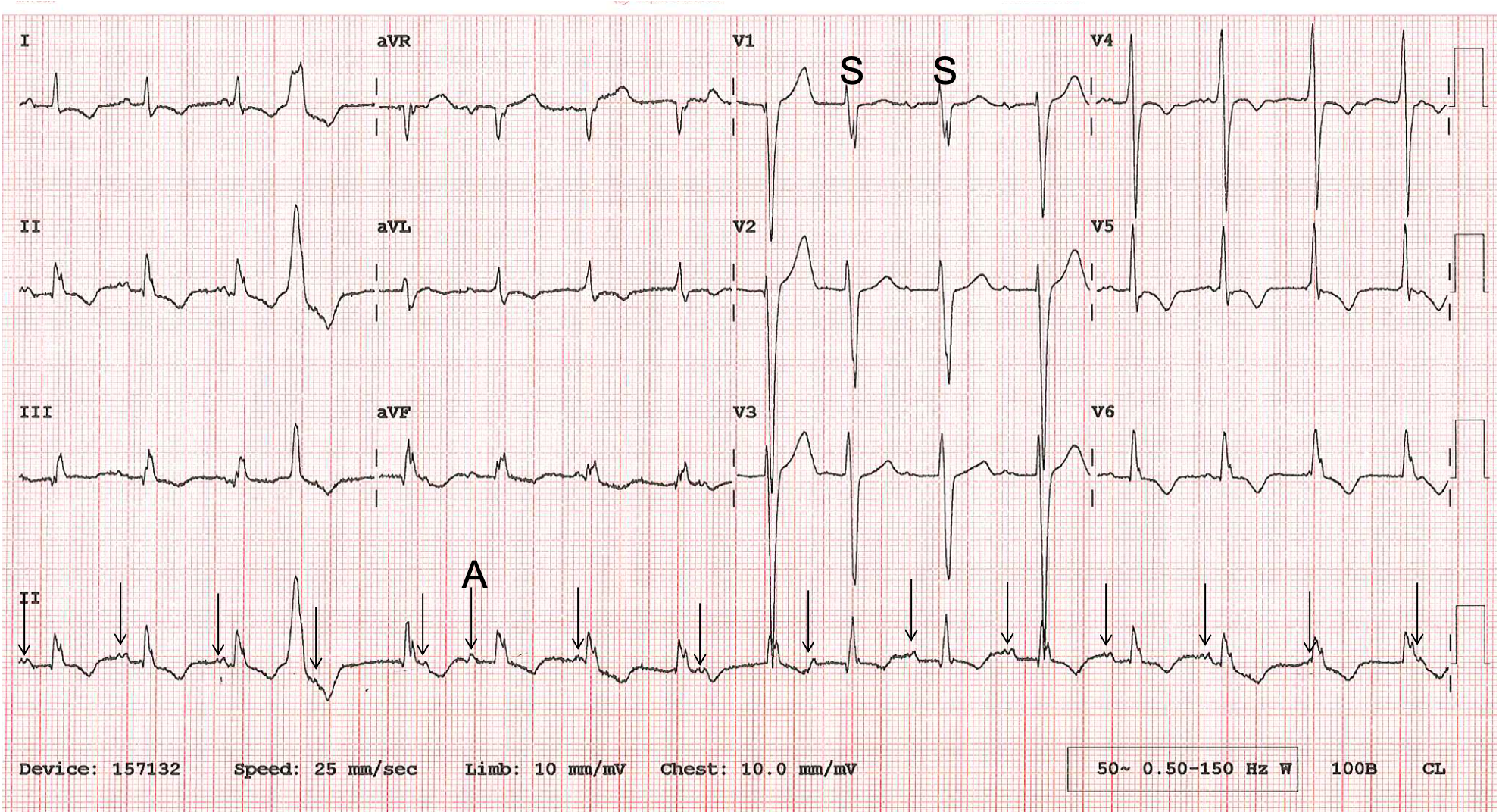
In summary, this is an accelerated junctional rhythm in the presence of an independent, slightly slower sinus rhythm, producing incomplete AV dissociation.
I think it’s an accelerated junctional rhythm with a slight intraventricular aberration pattern. Beat 4 is clearly a ventricular extrasystole. Beats 10 and 11 display normal AV conduction, albeit with a very slight partial RBBB and slightly long PR interval.
Both the ventricular extrasystole, and junctional beat that immediately follows it display retrograde conduction, causing a little irregularity in the otherwise consistent underlying atrial rate. There is also a little P-mitrale pattern (inferior leads), and biphasic (anterior leads) of the P-wave morphology.
Thanks, Scott. A great analysis as usual. I think I have a slightly different opinion over a couple of unimportant details, but I’ll provide my full explanation in a few days and perhaps we can then discuss the minor points of disagreement.