The rhythm here is irregular, but why? What exactly is going on? I’ve numbered the QRS complexes to facilitate discussion.
Dr Dave Richley,
Associate Lecturer
Newcastle University
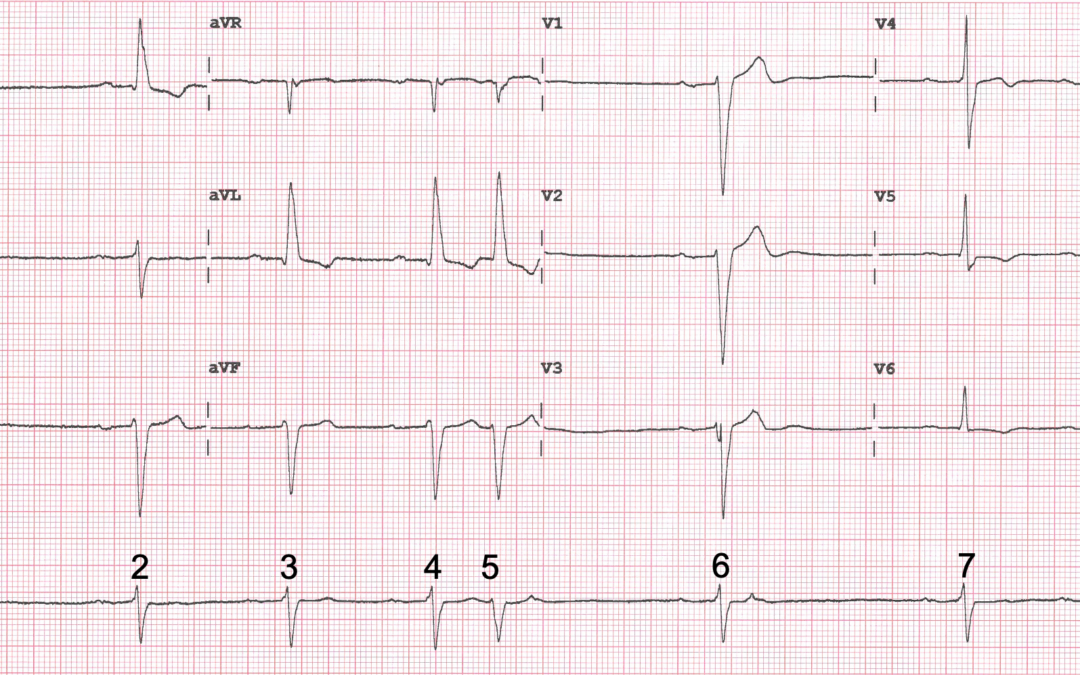
The rhythm here is irregular, but why? What exactly is going on? I’ve numbered the QRS complexes to facilitate discussion.
Dr Dave Richley,
Associate Lecturer
Newcastle University
Irregularity heart rhythm,Sinus bradycardia , 1st degree heart block, .left axis deviation = bifasicular block . Multifocal Atrial ectopics with compensatory pause,
HR ~30 bpm
I agree completely with you about the sinus bradycardia, left axis deviation and 1st degree AV block but I’m not sure that attaching the label ‘bifascicular block’ to this ECG is accurate or informative. First degree block is usually due to slow conduction in the AV node, which isn’t normally considered a fascicle. Bifascicular block is such an ambiguous term (LBBB, RBBB + LAFB, RBBB +LPFB, RBBB + long PR, LAFB + long PR etc) that it may be better not to use the term at all and simply describe the individual conduction defects, as has been recommended (1).
I also agree that there are atrial premature beats here, but my question is: where exactly are they? There may be more to this ECG than is immediately apparent.
Reference:
1. Surawicz B, Childers R, Deal BJ, Gettes LS. AHA/ACCF/HRS Recommendations for the standardization and interpretation of the electrocardiogram. Part III: intraventricular conduction disturbances. A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society.Endorsed by the International Society for Computerized Electrocardiology. Circulation. 2009; 119:e235-e240. DOI: 10.1161/CIRCULATIONAHA.108.191095
Sinus rate is actually around 55bpm, technically bradycardia.
First degree AVB, PR ~250ms.
Left axis deviation, with broad QRS, ~140ms, either left anterior hemi-block with LVH, or simply LVH giving rise to LAD.
We could define this as a non-specific intraventricular conduction delay, without relevant clinical history.
Premature complexes 5 and 9 have no preceding atrial activity, representing probable ventricular ectopy, with similar, but not identical QRS morphology. The P-wave in complex 5’s T-wave appears to be a red herring, and not truly retrograde; a coincidental nonconducted atrial extrasystole identical to that found in the following, normally conducted, sinus complex’s T-wave.
Complex 1 appears to be a genuine low junctional extrasystole, retrograde P-wave in ST segment.
If, as you say, the QRS width is 140 ms, then this would normally considered left bundle branch block rather than left anterior fascicular block, but the QRS shape isn’t typical of LBBB – the QRS actually seems to be of normal width in V6 – so maybe you’re right that it should be considered a non-specific intraventricular conduction delay. Now, are beats 5 and 9 definitely of ventricular origin? If you closely inspect the T wave of beats 4 and 8, do you think there might be a premature P wave on it? I’m not completely certain of everything we see here so I’ll examine the ECG some more and venture a full opinion next week.
The ECG shows:
Sinus bradycardia rate approx. 55 bpm
First degree AV block
Left axis deviation
Non-specific intraventricular conduction disturbance
Beat 5 is a ventricular ectopic
Non-conducted atrial ectopics hidden in the T waves of beats 5 and 6
Beat 6 is an atrial escape beat
Sinus bradycardia resumes with beat 7
I think the ECG shows:
• Sinus bradycardia @ 55 bpm
• First degree AV block
• Left axis deviation
• Non-specific intraventricular conduction defect
• Frequent atrial premature beats (APBs)
I think we’re all agreed on most of these points but what’s in question is exactly which are the atrial premature beats. My beat-by-beat analysis – which of course may be wrong – is a as follows:
Beat 1: seems to follow very shortly after a T wave, so may be an APB with its P wave superimposed on the preceding T wave. There is also a P wave in the ST segment of this beat and this may represent a 2nd consecutive APB, but one which is non-conducted. Alternatively, beat 1 may be a junctional premature beat with retrograde conduction.
Beat 2. A sinus beat.
Beat 3. Another sinus beat, demonstrating the underlying sinus bradycardia at 55 bpm.
Beat 4. A 3rd consecutive sinus beat but with premature P wave on its T wave (note slight T wave augmentation in lead II and increased terminal T wave negativity in aVR)
Beat 5. APB conducted with slight aberrancy, with a 2nd but non-conducted premature P wave on its T wave. This is therefore a pair of APBs, the 2nd one non-conducted.
Beat 6. Sinus beat with non-conducted APB visible on T wave.
Beat 7. Sinus beat
Beat 8. Sinus beat with premature P wave on T wave.
Beat 9. Aberrantly conducted APB.
Any other opinions?
Right, time for me to go into the garden and get some parsnips and brussels sprouts. Merry Christmas!
Beat 9 – Ventricular ectopic – which if it had been captured in the anterior chest leads I’m sure would be far more obvious. It’s appearance in V4 is clearly very different from the native QRS yet similar in duration. With such a broad QRS already, how much more aberration is actually possible without increasing the QRS duration?
With existing slow AV conduction, and the non-conduction of the obvious premature atrial complexes, the supposed P-waves for beats 5 and 9 would have to be within the preceding QRS or ST segment – and hence too premature to be conducted, as those seen in preceding T-waves (which are less premature) were not conducted. This is all about absolute physiological refractory periods, not even the complicated relative ones.
And I believe J.Rankin was possibly correct about the atrial escape beat too – although viewed this using Internet Explorer as has failed to comment on Complex 9 (the other ventricular ectopic) – Google chrome shows the full image.
Merry Christmas indeed.