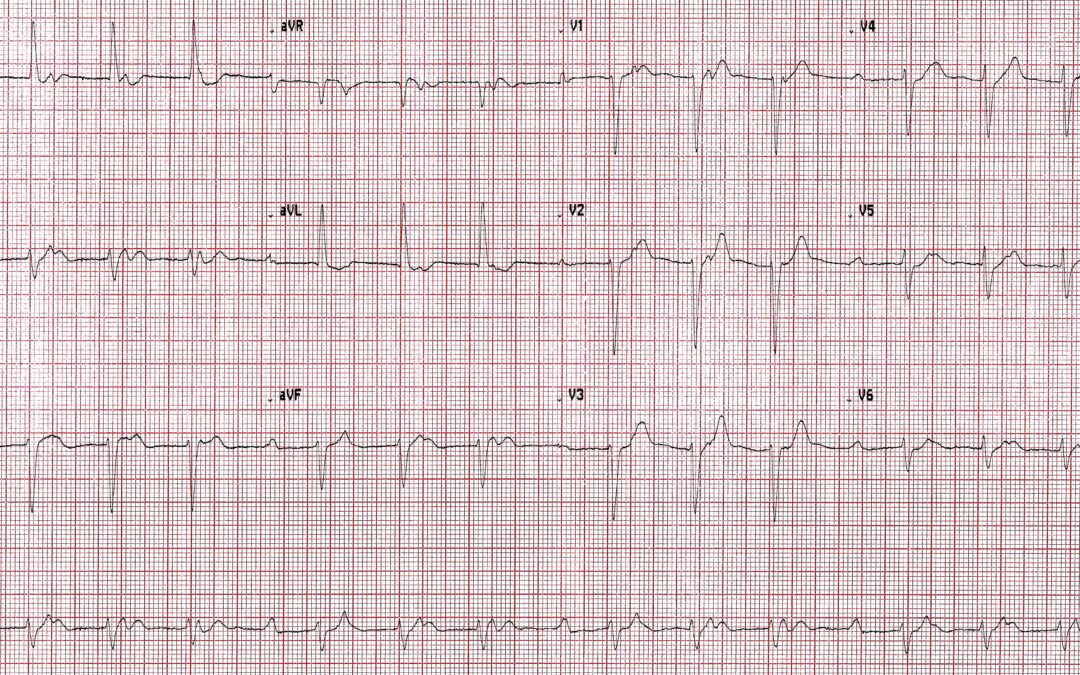
Let’s start the year with an easy one. The quality isn’t as good as I’d like but it’s good enough for answering the question: what is the rhythm? This is one that might not be obvious at first glance but a careful analysis should yield the correct answer.
Answer
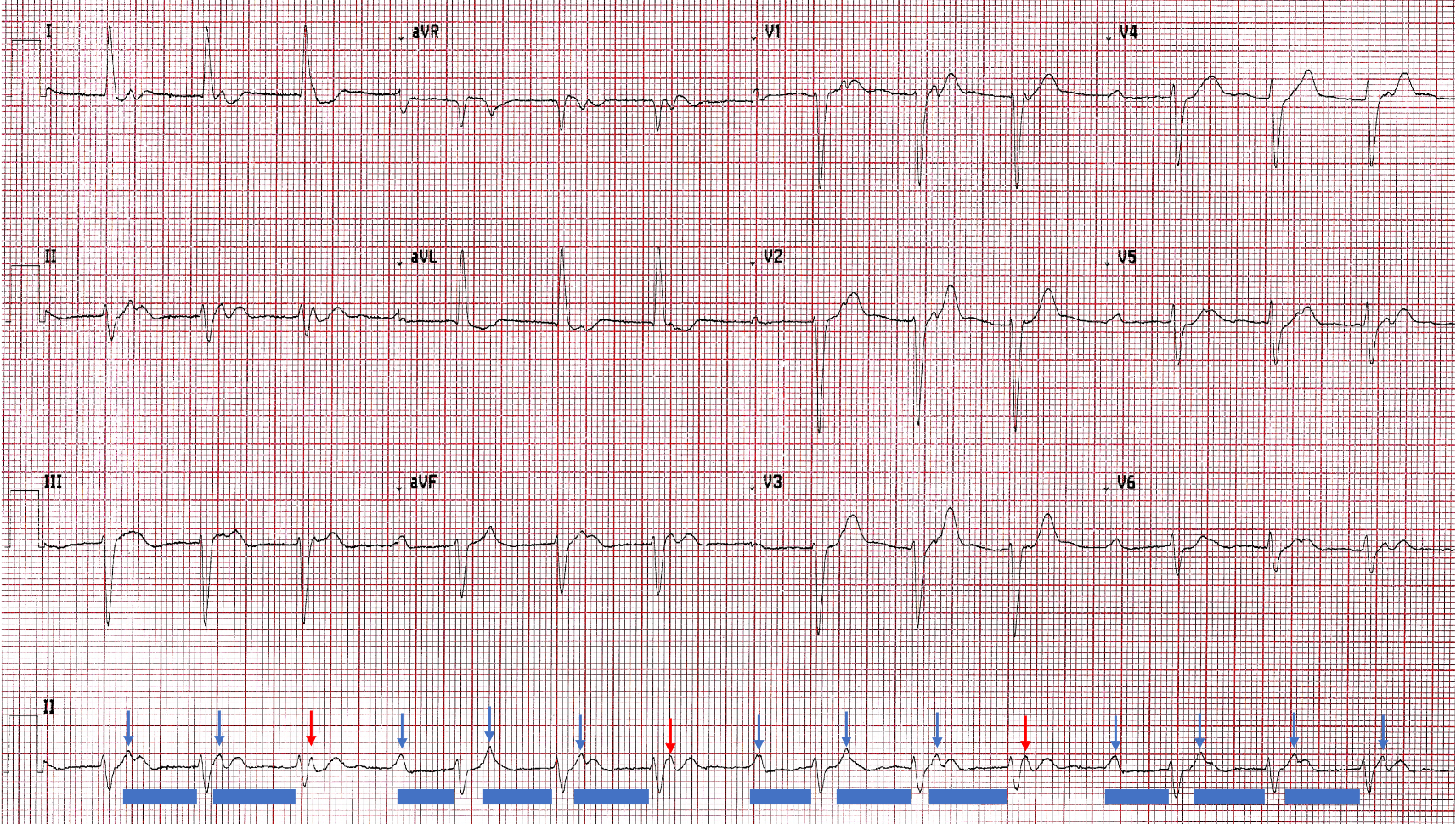
This one is not complex but it’s easy not to recognise straight away what is happening. The key, as so often with arrhythmias, is first to identify the atrial activity. I’ve shown the P waves below with arrows and it’s now clear that there is an underlying sinus rhythm/tachycardia and that not all P waves are followed by a QRS complex. I have also shown the PR intervals with blue bars, and it should now be apparent that there is 4:3 Wenckebach AV block. The red arrows show the blocked P waves.
This is a simple rhythm disturbance but what makes it perhaps difficult to recognise immediately is the length of the PR intervals: the shortest is 440 ms, the longest 600 ms. As we have seen before, when the PR interval is very long it is difficult for the human/eye brain combination to make the link between P wave and QRS. However, when the P waves are clearly marked, as here, the relationship between P and QRS is much easier to appreciate.
Well done to those who worked it out. As Scott Walton and Arron pointed out, there is also a left axis deviation that is most likely due to left anterior fascicular block.
Sinus rate of around 90bpm. Mobitz I conducting around 72bpm. LAD and non-specific poor R wave progression also present.
Re-entrant Accelerated Junctional Rhythm ~92bpm, P-waves present after each QRS complex..
Thanks to Maison and Jon for their very different explanations. Does anyone agree or disagree with either of them or have any other comments to make?
Agree with accelerated junctional rhythm with retrograde p-waves, with a rate of 90 beats per minute, ?Possibly a high-grade second-degree heart block (4:3)
?Non-conducted p-waves ( 4th,8th,12th ) on the strip. LAD
Thanks Camilla. You offer us a couple of alternative explanations – do you have a clear preference?
Wenckebach with concurrent 1st degree and left anterior fascicular block.
Thanks, Scott. So, are there any other opinions out there or have we exhausted the possibilities with this one now?
Sinus rhythm with 2nd degree AV block Mobitz I/Wenckebach (4:3 conduction) – the P wave axis is normal so we know that these P waves are not conducted retrogradely.
Left axis deviation with clockwise cardiac rotation indicating Left Anterior Fascicular Block
R wave in aVL ~13 mm which may raise suspicion of LVH too however there is a left axis deviation so perhaps this is less reliable? Then again there are ST-T abnormalities in I and aVL with further raises the possibility of LVH. I have seen a voltage criteria for measuring the R wave in aVL when there is left axis deviation however I am unsure of its reliability.
When await Dave’s insightful comments.
Great comments Arron – thanks. It is a long-held convention that an R wave amplitude of at least 11 mm is not indicative of LVH when there is LAFB, but there is recent evidence to the contrary, so I’m not sure what the truth is. I certainly wouldn’t rule LVH out here, but then I don’t think I would ever rule out LVH on the basis of the ECG alone.