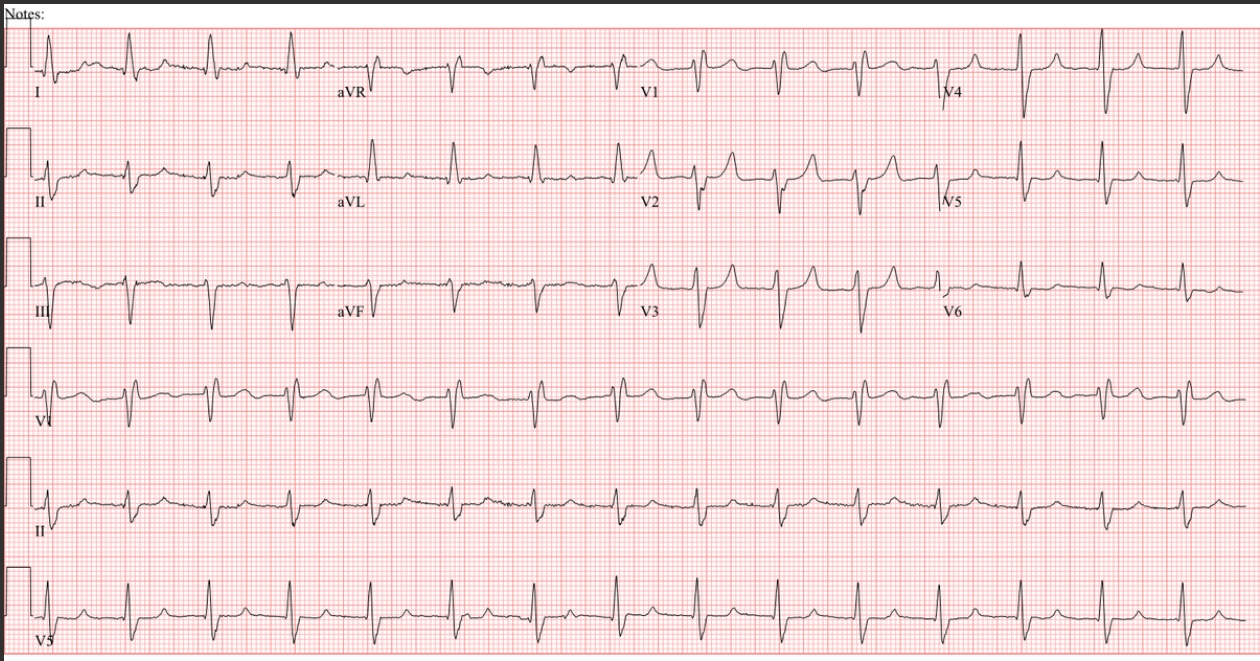
For this month’s ECG I am indebted to Esta Felix, 1st year STP trainee at Somerset Foundation Trust and MSc cardiac science student at Newcastle University. The question here is: what is the rhythm?
The patient is a 75-year-old male with a dilated cardiomyopathy who had undergone ablation for atrial fibrillation. He has also been implanted with a CRT pacemaker. Can you work out the rhythm with confidence from this ECG or is there more than one possibility? If the latter, what are the possibilities, and what additional information might help you to decide which explanation is correct? After there has been some initial discussion, I will post another ECG from the same patient.
Dr Dave Richley
Further Comment Added 21.05.24
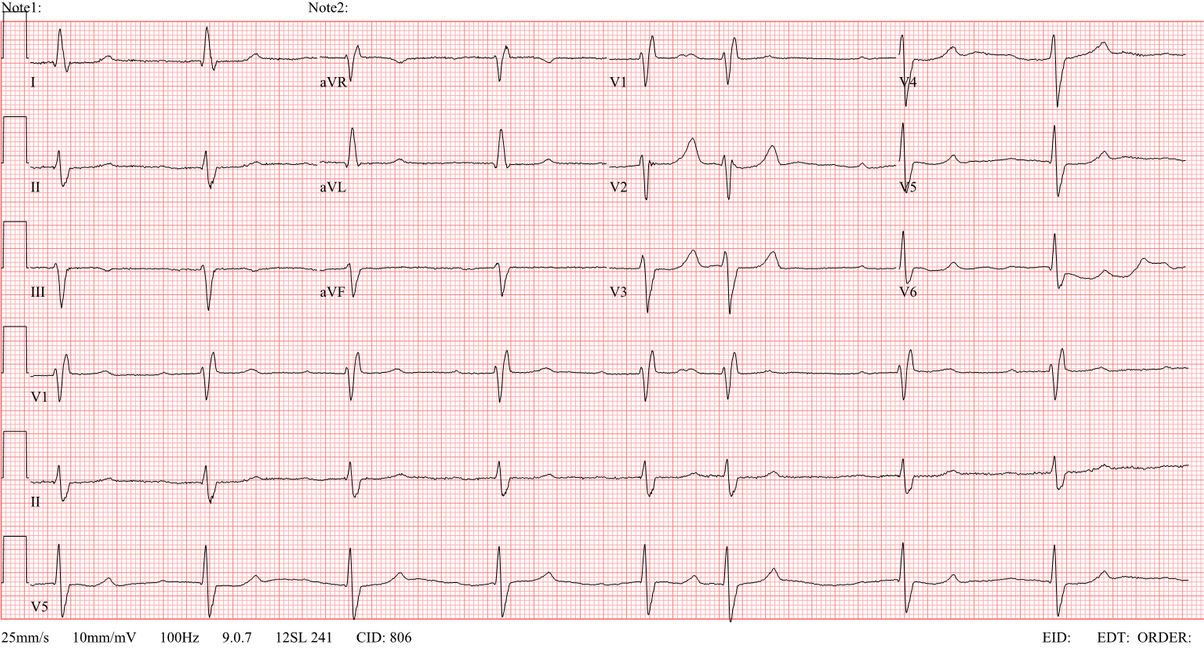
Unable to decide with confidence what the rhythm was, I asked if there were any other recordings and luckily Esta managed to supply one. I think this ECG makes everything clear. Any comments?
Answer Added 28.05.24
When I first looked at the original ECG I thought it might be an example of accelerated idioventricular rhythm (AIVR), that probably, because of the left axis deviation/right bundle branch block pattern, arises from the left posterior fascicle. But I was troubled by the apparent absence of atrial activity: in an AIVR it is usual to see either AV dissociation because of an independent sinus rhythm, or a negative P wave after each QRS owing to retrograde conduction over the atria. So then I wondered if this might be sinus rhythm with first degree AV block, left axis deviation (possibly due to left anterior fascicular block) and right bundle branch block, with the PR interval so prolonged that the P wave coincides with the peak of the T wave and is therefore not clearly visible. To resolve this diagnostic dilemma I asked if Esta had another recording, hoping that if this was the case the ventricular rate might be different and all would be clear. The second ECG shows a sinus bradycardia, again with left axis deviation and right bundle branch block, and because the sinus rate is slower on this ECG the P wave no longer falls on the T wave and is easily seen. There is also one atrial premature beat, in which the premature P wave falls on the T wave of the preceding beat, mimicking the situation in the first ECG where the P waves were difficult to visualise. Therefore, the original ECG showed sinus rhythm with first degree AV block, left axis deviation and right bundle branch block – NOT an accelerated idioventricular rhythm. Sometimes, as in this case, multiple recordings can help in elucidating a rhythm.
Dr Dave Richley
AF, Left Axis deviation, CRT ?LBP
We have a regular rhythm with RBBB and LAHB pattern. No overt atrial activity, although I think the p-wave is engulfed in the t-wave, making this what is typically called “trifascicular” block, first degree + bafascicular.
It could also be a junctional or idioventricular rhythm if the p-waves aren’t present; hopefully his CRT stores ventricular sensing episodes, as interrogation may interrupt the rhythm preventing assessment of the real-time EGMs. I’m assuming a dual chamber device, with failed tracking due to PVARP lock-in.
Thanks, Scott. An astute analysis, as usual. Has anyone else got any comments?
I’ve gone back and forth with this ECG for a little while. My first gut instinct, in the first few seconds of reading the information and glancing at the ECG, was 2:1 flutter or AT.
I then considered Sinus rhythm, AJR, AIVR (from the LPF), atrial pacing, ventricular pacing etc.
The rate is around 90bpm throughout with typical RBBB and LAFB morphology. There are some deflections (namely lead I and beats 6 and 7 in V5) I thought could be atrial activity but after some crude mapping, I conclude that they are probably artefact. The T waves have a notched appearance which make us consider hyperkaelemia and P wave superposition. The possibility of Hyperkaleamia draws me back to AJR but this seems unlikely. The T wave morphology in certain leads look very suspicious for P waves hiding in the T waves. That being said, subtle changes in RR usually reveal the hidden P waves out of the T waves, but I don’t see see evidence of this.
I cannot see any clear evidence of pacing and the QRS morphology looks typical for “native”/Supraventricular conduction, making pacing unlikely.
If we were to consider Bix’s rule, we should see extra P waves at the very start of each QRS (based on my crude mapping). However, I cannot see any clear evidence of these “extra P waves” (some cases the P waves are fully hidden in the QRS waveforms but I think they would map to very start of the QRS).
AIVR from LPF seems unlikely given the history and typical bifascicular block morphology.
In summary im not 100% sure but suspect this may be Sinus rhythm with 1st AVB, LAFB and RBBB. Some vagal manoeuvers, if appropriate, may confirm my suspicion that this is sinus rhythm.
Looking forward to Dave’s insightful comments.
Thanks, Arron – I’m glad I’m not the only one who agonised over this one! Ultimately I was unable to decide between 2 alternative explanations so I asked if Esta had any other recordings that might help to clarify things. Luckily she managed to supply one, and I was able to resolve my dilemma. I’ll get this posted soon, so look out for it.
Hi Dave. Any possibility for bix rule here thinking in AT/AFL? Was my first dx. Thank you.
Thanks for the question, Javier. I don’t think the Bix rule applies here because according to my measurements the QRS is not midway between 2 visible P waves. it’s something that always has to be considered, though.