I have been trawling my archives and come up with what I think is a challenging case involving three ECGs. Personal and clinical information has been minimised in order to preserve patient confidentiality and anonymity.
Figure 1 is the initial ECG of a young boy, and figure 2 an ECG recorded from the same boy three years later. Figure 3 is the initial ECG of the child’s brother.
What abnormal features can you see? What diagnosis do these features suggest?
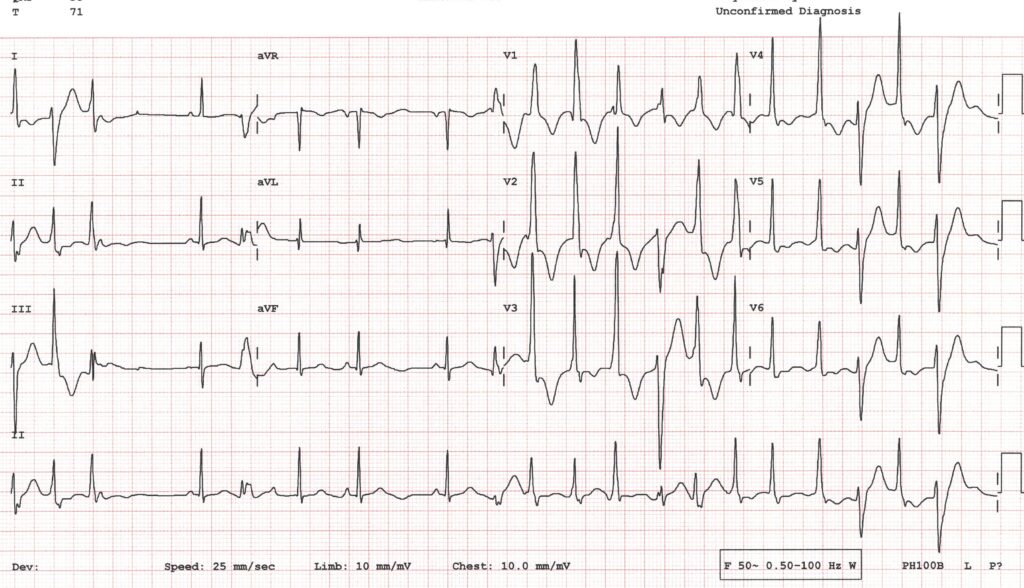
Figure 1 – Initial ECG of boy 1
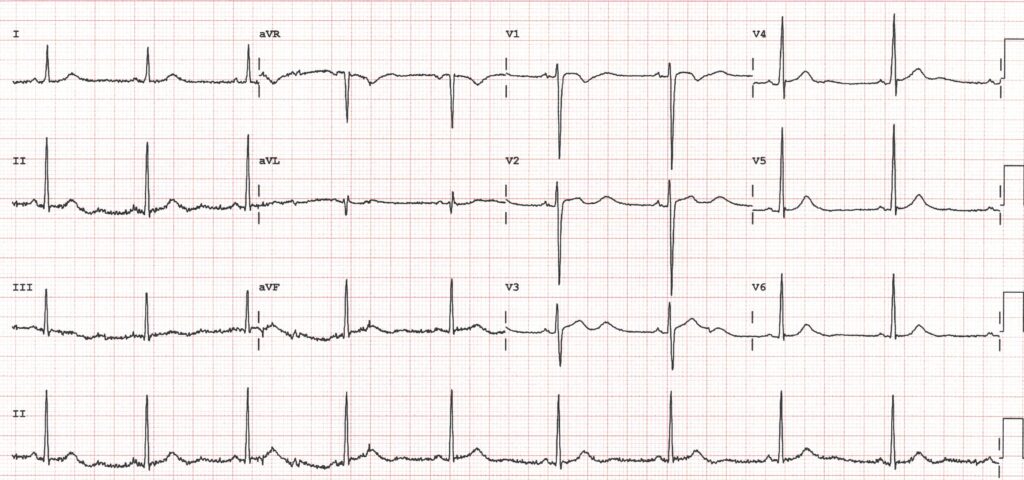
Figure 2 – Boy 1’s ECG 3 years after initial presentation
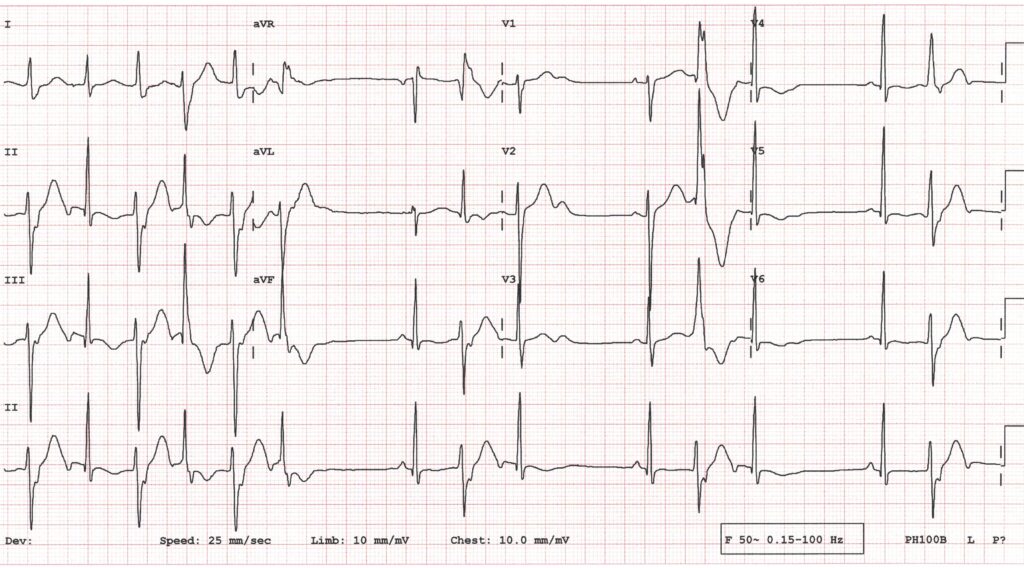
Figure 3 – Initial ECG of boy 2, the brother of boy 1
ANSWER
These ECGs are from a family with Anderson-Tawil syndrome (ATS), a rare inherited condition in which there is a potassium ion channel abnormality. The three main features of the syndrome are:
- Episodic muscle weakness (periodic paralysis)
- Distinctive facial and skeletal dysmorphia
- Ventricular arrhythmias, which may be lethal
ATS used to be considered a variety of long QT syndrome (LQT 7), but is now thought of as a separate entity because the QTc is usually normal. The most commonly reported ECG abnormalities in ATS are:
- Prominent U waves, particularly in V1-V4 and the limb leads. This is different from the situation in normal individuals, where it is rare see U waves in the limb leads. Also, in the normal population, U waves are often only seen in sinus bradycardia whereas in ATS the size of the U waves often increases with the heart rate.
- A prolonged QU interval. In normal individuals it is common for the beginning of the U wave to overlap with the end of the T wave but in ATS the 2 waves are often completely separate which prolongs the QU interval.
- Biphasic U waves
- Ventricular premature beats in which the T wave fuses with a large U wave to produce a very broad deflection.
- Frequent, polymorphic ventricular ectopy at rest. This is in contrast to what is seen in long QT syndrome and catecholaminergic polymorphic ventricular tachycardia, where the ventricular arrhythmias are typically provoked by exertion.
In figure 4 I have highlighted some of the characteristic ECG features of ATS from the 2 family members in this case.
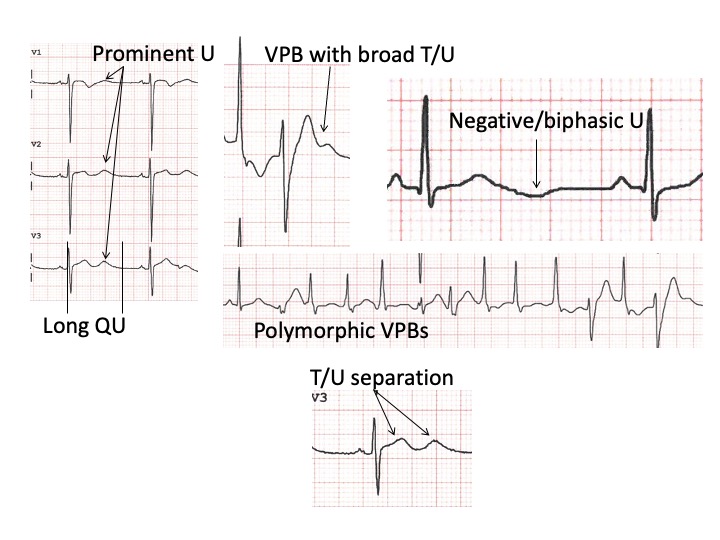
Figure 4. Some of the ECG features of Andersen-Tawil syndrome that are seen in 2 family members.
Well done to wangchangkun for recognising the ECG pattern so quickly.
The amplitude of the u wave increases,There is also BVT performance.Suspected to be Andersen Tawi syndrome
Thanks, wangchangkun. I’ll reply in detail after others have had the chance to offer their interpretations.
I’d be suspicious of CPVT
Thanks, Joy. I’ll provide a full explanation in a few days’ time.