This ECG was recorded from a 20-year-old male who collapsed after experiencing palpitations while travelling on a bus. Are there any abnormal features that suggest a possible cause of the symptoms?
The Answer
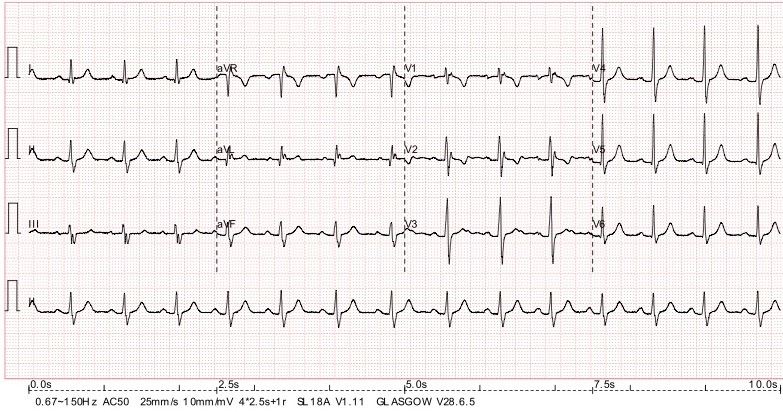
The most unusual feature of this ECG is what looks like a second, small R wave in V1 and V2. As Adi and Mags point out, these deflections may be epsilon waves due to arrhythmogenic right ventricular cardiomyopathy (ARVC). ARVC is a disease in which RV myocytes separate from each other because of faults in the proteins of the desmosome, the ‘adhesive’ junction that binds the cells together. This process results in patches of right ventricular myocardium becoming progressively replaced by fibro-fatty material and this produces heterogeneity in ventricular depolarisation with affected areas subject to prolonged and delayed electrical activation. This may cause a prolonged upstroke of the S wave and/or additional small positive deflections – epsilon waves – just after the QRS in leads that face the right ventricle, ie mainly V1 and V2. Typically, these leads also show T wave inversion. The main problem with ARVC is a propensity for ventricular tachycardia and subsequent sudden death. The VT, because it originates from the right ventricle, typically has a left bundle branch block morphology.
It is now known that the cardiomyopathic process just described also affects the left ventricle in most if not all cases, and for this reason the condition is increasingly being termed ‘arrhythmogenic ventricular cardiomyopathy’ (ACM). Significant left ventricular involvement may be inferred by the presence of more widespread T wave inversion.
It is important, to spot these abnormalities on the ECG and understand their possible implications in the context of the clinical presentation so that further, definitive, investigations can be undertaken. In this case, the patient was referred for further investigations but we do not have the results of these, so we cannot say for certain that the patient had ARVC.
I am grateful to Sam Bean for sharing this ECG with me.
My first thought was there was “spike” on the ST-segment of V1 which also had T-wave inversion. This can also be seen on V2 and 3. On closer inspection aVL also has a notched J-point, and there are notches in the S-waves of the inferior leads.
Are these epsilon-waves? If so then ARVC would be the diagnosis. I think ARVC is usually discovered when the patient is a young adult, and can cause palpitations with syncope because of the increased risk of VT.
Isn’t it associated with a specific “lower risk” type of VT? I can’t remember the name at the moment.
I agree with your diagnosis Adi. I seem to remember there is a way of recording bipolar chest leads which shows it up better. Fontaine positions.
Thanks, Adi and Mags, for your comments. I won’t say anything about the ECG yet. Any more views out there? Do people agree or disagree with what’s been said so far, or have anything to add?